| Theories and Techniques of Oral Implantology (vol.2) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
610 Theories and techniques of oral implantology
dense connective tissue close to the implant. Within 2 or 3 months, a large radiolucent area can be seen around the spiral portion of such an implant (Fig. 14-1).
As a rule, when less than 5 mm. of alveolar bone height exists, it is inadvisable to use a post type implant. A blade-vent, whose stability depends on its anteroposterior length rather than its depth, can be often used in a shallow area. However, enough bone must remain to bury the implant's shoulder, or epithelial invagination does occur (Fig. 14-2) .
In addition to adequate bone height, there must be adequate bone width. Narrow ridges are unsuitable for post type implants, since there also must be sufficient bone around an implant to hold it secure. Fortunately, blade implants can now be used in such situations.
When faced with a case where little bone exists between the alveolar crest and a sinus or the mandibular canal, a triplant is often recommended. Be-
cause the stability of such an implant depends on diverging the legs as far apart as possible, the danger of perforation is particularly great (Fig. 14-3). Great care must be taken in evaluating the most advantageous positions for triplant pins. If one of the pins perforates the bone, the triplant becomes less stable.
Unhealed extraction sites
Unhealed extraction sites, or open sockets, should be avoided. The bone in such an area is in a state of flux. Unless the implant can extend beyond the apex of the socket into an artificially made one and can be splinted to a tooth on each side, which would provide the stability needed for normal healing, an open socket is an undesirable site. Post type implants in open sockets usually fail (Fig. 14-4). Implants placed too near sockets also tend to fail (Fig. 14-5).
When desiring to substitute a recently lost tooth,
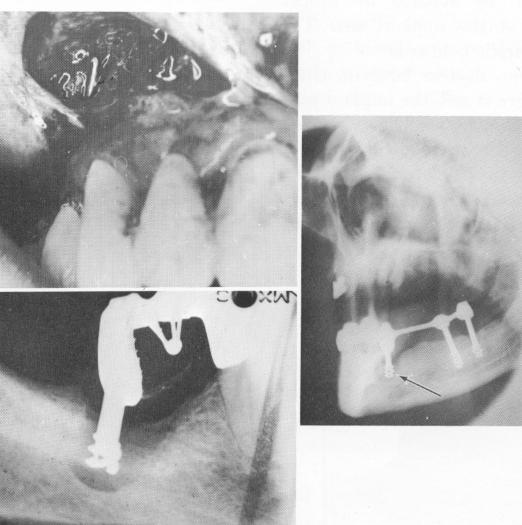
A
B
C
Fig. 14-4. A, A pin implant perforating the labial plate of bone is seen by incising and retracting the mucoperiosteal tissue. B, Post type implants must not be placed into recent sockets unless they can be set beyond the floor of the socket into a deeper artificial one and immediately stabilized with a prefabricated fixed denture. Otherwise a rapid epithelial invagination takes place directly into the sockets, preventing future bone regeneration. (From Linkow, L. I.: Alloplastic implants. In Goldman, H. M., Forrest, S. P., Byrd, D. L., and Mc-Donald, R. E.: Current therapy in dentistry, vol. 3, St. Louis, 1968, The C. V. Mosby Co., pp. 335-356.) C, Another post type implant failing in an open socket. If no bone in the floor or the walls of the socket is available for some part of an implant, the intervention should be delayed until the bone heals.
|
|
Page 610 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|