| Theories and Techniques of Oral Implantology (vol.2) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
Causes of implant failure 609
sincere desire to correct their detrimental habits may be acceptable candidates.
Whatever the reason for implantation, the role of good oral hygiene after implantation and the reasons for it should always be explained to any candidate. The dentist who knowingly performs an implantation on a candidate with consistently poor oral hygiene habits or the dentist who fails to stress the importance of proper hygiene should not be surprised if postoperative complications arise.
Periodontal disease should be cured, or at least controlled, before implantation and its causes corrected or alleviated. If poor occlusion has resulted in pockets or abscesses around remaining natural teeth, it certainly will not help a dental implant. Here common sense dictates: periodontal problems leading to the eventual loss of natural teeth will also lead to the loss of dental implants.
Poor site selection
Many of the problems arising during endosseous implant interventions can be avoided by proper selection and evaluation of the implant site. The following observations generally hold true.
There must be sufficient alveolar bone in which to bury the implant. If there is not, the implant may impinge upon the mandibular canal, maxillary sinus, or nasal vestibulum. Errors here will cause, at the very least, sensitivity or pain. At most, facial paresthesia caused by nerve damage can occur.
When too little alveolar bone height remains and if post type implants are used, the implants may
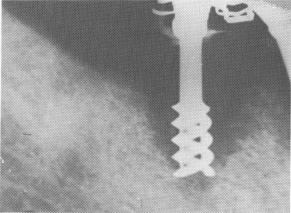
Fig. 14-1. Bone resorption rapidly occurs where the open spirals are not deeply buried in the bone. In this case, a rapid invagination of the epithelium through the spirals that were near the alveolar crest took place, preventing the bone regeneration from growing closer to the implants. (From Linkow, L. I.: Clinical evaluation of the various designed endosseous implants, J. Oral Implant Transplant Surg. 12:35-46, 1966.)
eventually fail because of soft tissue invagination. A 2- or 3-mm. invagination is harmless, providing that the narrow abutment post, not the open spirals, is embedded in the area. Otherwise a rapid invagination of the epithelial tissue occurs in and between the spirals, preventing the regeneration of bone or
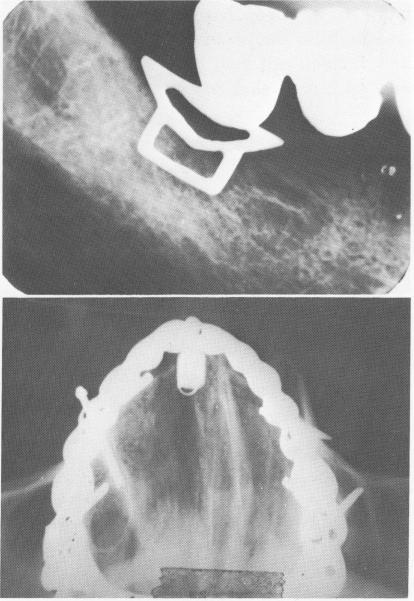
Fig. 14-2. The typical V-shaped breakdown of bone associated with soft tissue invagination is exemplified by this case.
Fig. 14-3. A, Bone resorption also occurs when the shoulder of the blade implant is not buried below the alveolar crest of bone. B, A cross-sectional x-ray reveals perforation of the labial and buccal plates of bone with pin implants, which often can occur. (From Linkow, L. I.: The era of endosseous implants, J. D. C. Dent. Soc. 42 [2] :14-19, 1967.)
A
B

|
|
Page 609 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|