| Theories and Techniques of Oral Implantology (vol.2) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
584 Theories and techniques of oral implantology
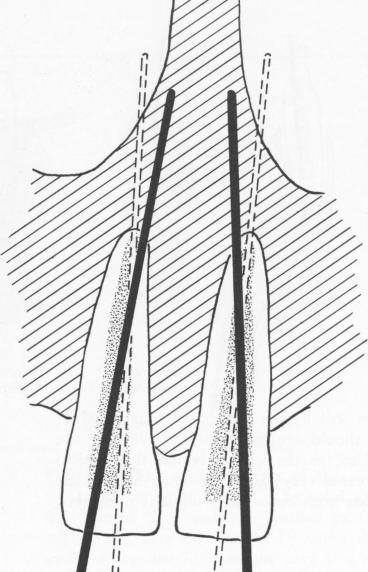
Fig. 13-3. The pins may be angled to lodge in the nasal spine and septum. This permits using longer pins than could otherwise be used if the axes of the root canals were followed (dotted lines). To angle a stabilizer toward the nasal spine, the root canal must be enlarged distally at its crown and mesially at its apex. (Redrawn from Orlay, H. G:. Splinting with endodontic implant stabilizers, Dent. Pract. (Bristol) 14[2]:481-491, 1964.)
(Fig. 13-3). Another method of gaining more sup-port in bone is to widen the canal lingually so that the axis of the alveolar process may be followed (Fig. 13-4).
In dealing with roots with bends, the opera-tor should resort to intentional perforation. Of course, that part of the canal apical to the perforation must be previously sealed with gutta-percha. Such teeth seem to be particularly well stabilized, having been made "two-rooted" by the operation. As for multirooted teeth, they can be extremely well secured by placing an implant in two or three roots.
The problem of reconciling the optimum direction of an implant with tooth anatomy will lessen as the operator gains experience.
TOOLS AND MATERIALS
Provided that the operator has the usual endodontic and periodontic equipment, only a few new
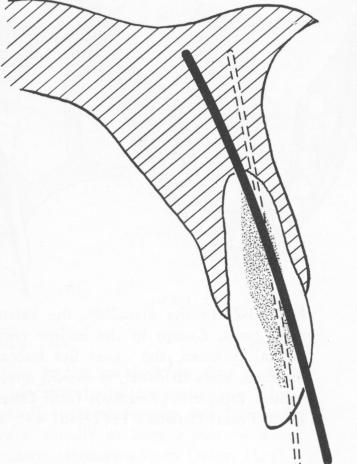
Fig. 13-4. Angling the pin along the axis of the alveolar bone (solid line), rather than along the axis of the root canal (dotted line), often gives greater stability. (Redrawn from Orlay, H. G.: Splinting with endodontic implant stabilizers, Dent. Pract. (Bristol) 14 [2] :481-491, 1964.)
tools and materials are needed for endodontic implantations.
Stabilizer pins. Four standard endodontic implant stabilizers are suitable for most cases. They are all 60 mm. long, the thickest tapering from 2 to 1.25 mm., the thinnest from 1.25 to 0.7 mm. (Fig. 13-5). Assuming that threaded pins might provide a greater hold in bone, some operators have tried them (Fig. 13-6). However, the threads are too close together to allow bone to grow between them, and the only advantage of the threaded pin is that cement adheres somewhat better to it.
The metal of which the implant is made must be biologically compatible with the tissues in which it is set. Results with the chrome-cobalts Virilium and Vitallium have been very good. Certain titanium alloys, such as Plantanium* (with and without sapphire coating), have been excellent. Although tanta-
*Manufactured by Implant Research Corp., Pennsaukin, N. J.
|
|
Page 584 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|