| Theories and Techniques of Oral Implantology (vol.2) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
Endodontic implants 583
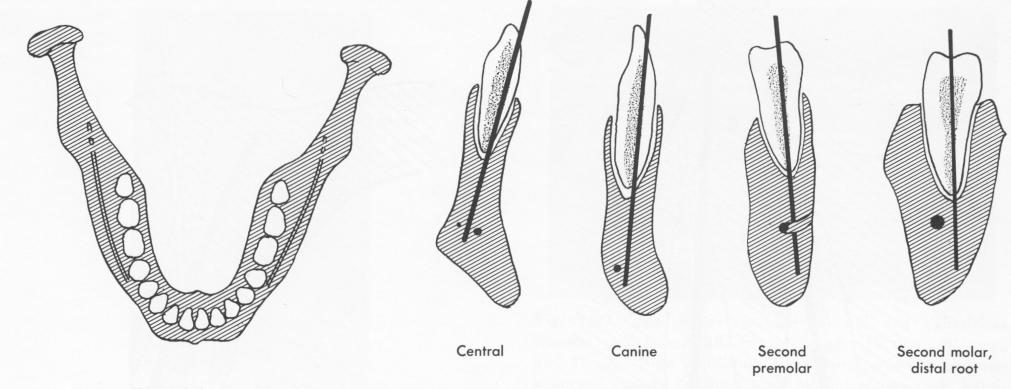
Fig. 13-2. In the mandible, the extension of root axes will bypass the mandibular canal in most cases. Except in the incisor region, if the canal should continue anteriorly beyond the mental foramen, the canal lies buccal to the axes. Also, in the incisor region the vertical distance, apex to canal, is usually great. However, the canal very rarely continues beyond the mental foramen. (Redrawn from Orlay, H. G.: Splinting with endodontic implant stabilizers, Dent. Pract. (Bristol) 14 [2] :481-491, 1964.)
rules and consequent suggestions for varying their applications. The primary rule is that the implant should extend into the bone as deep as is anatomically possible; the denser the bone, the better the stabilization. In the maxilla, the amount of bone between the apex of the tooth and the nasal cavity or the maxillary sinus is the main factor determining the possibility of implantation and the probability of success. The more bone height present and the smaller the cavity, the greater the success rate. How-ever, even in unfavorable cases sufficient bone usually can be found by utilizing the nasal spine, the front parts of the septum, the canine prominence, the triangular mass of bone on the palatal side of the incisors, and sometimes even the zygoma and the tuberosity (Fig. 13-1).
Perforation of the maxillary sinus by a pin implant should naturally be avoided. Although the ciliated epithelium will tolerate the emerging post in the same manner as the stratified oral epithelium will tolerate the emerging cones of prosthodontic implants, the pin will be unstable. A protruding post will irritate the nose, and crusts of dry mucus will accumulate around it.
Two areas of compact bone are visible on occlusal radiographs of the mandible. The implant posts should reach at least one of these areas, if not penetrate right into it, to give the end of the post a firm grip.
There is very little danger of injury to the mandibular nerve in endodontic implant stabilization. The mandibular canal lies lateral to the alignment of the teeth (Fig. 13-2). The small branches of the nerve are rarely harmed. Because those fibers serving the lips and gingivae leave the bone at the mental foramina, they are usually well out of the operatory site.
Although it is not necessary when inserting endosseous or subperiosteal implants, the operator wishing to insert an endodontic implant must contend with tooth anatomy. One of the most important considerations is the direction of the root canals. The axes of root canals do not coincide with the axes of the crowns of the teeth. This frequently makes it necessary to enlarge the root canal considerably to accommodate the rigid post. Sometimes parts of the incisal edges or even of the labial surface of a tooth must be sacrificed for this purpose.
Often, the direction in which the pin should be inserted for maximum support in bone does not correspond with the direction taken by the axis of the root canal. Sometimes this is easily remedied by enlarging the canal. In an upper central incisor, for example, the coronal part of the canal may be enlarged distally and the apical area mesially. This alters the ultimate direction of the post so that it becomes embedded in the nasal spine, permitting better fixation through the use of a longer implant
|
|
Page 583 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|