| Theories and Techniques of Oral Implantology (vol.2) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
582 Theories and techniques of oral implantology
Small sinus
Large sinus
Large sinus
Small sinus
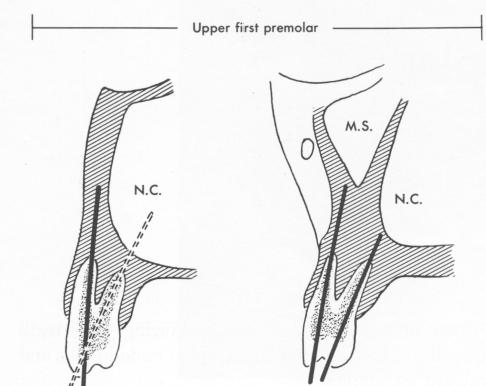
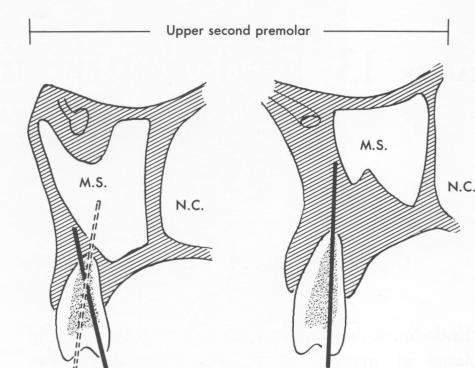
Fig. 13-1. The extended axes of the root canals in relation to the nasal cavity (N.C.) and the maxillary sinus (M.S.). The solid axes indicate ideal placement sites for endodontic pins. The dotted lines indicate possible perforation of a sinus. Even if these axes are followed, perforation may be avoided by using shorter pins. There is usually at least 5 mm. of bone available for the intraosseous part of a stabilizer in such cases. (Redrawn from Orlay, H. G.: Splinting with endodontic implant stabilizers, Dental Pract. (Bristol) 14[2]:481-491, 1964.)
radically from those of other implants. At first the debris of the operation will be resorbed, and later a very thin layer of fibrous tissues, about 2 to 3 cell diameters thick, will surround the implant in the reorganized bone. One investigator, experimenting with dogs, reported finding layers of epithelial cells of Malassez around the deeper part of his implant. This could be theoretically possible where epithelial tissue has invaginated down to the apex of the tooth. In this situation by perforating the periodontal membrane to set the implant deep in bone, some epithelial cells might be carried down into the bone and proliferate there. However, the presence of these cells seems to be of no practical clinical importance.
EVALUATING THE CANDIDATE
The probable success or failure of any type of surgery depends upon the patient's general health, local conditions, and attitude. As has been extensively discussed previously, the patient's general health should be good. Any systemic condition, particularly involving the blood or bone, that might affect healing should contraindicate the procedure. When the implantologist is in doubt about the patient's general health, he should consult the patient's physician.
Periodontal conditions
The dentist is the best judge of local conditions. Obviously, only patients who carry out proper oral hygiene should qualify, and all should be instructed how to brush the teeth and otherwise care for the mouth after the procedure.
About 80% of all presenting patients have teeth loosened by periodontal disease. Of these, two-thirds involve the lower front teeth. Periodontal disease, except in very advanced cases, is not a contraindication. As long as at least 3.5 mm. of viable periodontal membrane is visible on a radiograph, the operation is possible.
It is difficult to advise whether periodontal treatment should precede or follow the endodontic implantation. Each case must be determined by its particular circumstances. Generally speaking, very loose teeth should be stabilized first; otherwise they may become too weak for any treatment. But whether before or after implantation, all periodontal treatment necessary must be performed for long-term success.
Anatomic considerations
Although the anatomy of the jaws differs a great deal from patient to patient, there are a few general
|
|
Page 582 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|