| Theories and Techniques of Oral Implantology (vol.2) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
544 Theories and techniques of oral implantology
Fig. 12-28. Icepacks are placed inside a towel in the neck and chin area and tied around the top of the patient's head.
tissue that has either never been operated upon or not operated upon for many years. There is a fairly good blood supply, which allows for rapid healing of the wound. Another important factor at the first surgical stage is that the tissues are merely joined together and do not have to be stretched over an implant, as is done during the second stage. Also, during the first stage the fibromucosal tissue is very widely reflected in order to expose enough of the bone for a bone impression. This makes this tissue more mobile for suturing.
Healing after the second surgical stage is more complicated. Scar tissue has developed all along the original incision site and in the approximating tissues. Scar tissue has a greatly reduced blood sup-ply, and its fibrous tissue content is greatly increased. It is into this avascular bed of scar tissue that the second surgical incision is made. Because of this lack of an adequate blood supply, the healing over the implant is retarded and could take place by secondary intention, or healing by granulation tissue. This is less desirable because granulation tissue cannot be con-trolled, and the tissue never adheres as closely to the protruding posts as it does with healing by primary intention.
Several techniques have been tried to compensate for or alleviate the problems associated with the second surgical stage. The amount of time between the first and second stages has been increased to as much as 2 months to allow for complete cicatrization across the original incision. Some operators re-strict the amount of tissue reflected, thinking that this helps reduce postoperative swelling, pain, and edema and speeds healing. Just enough tissue is in-
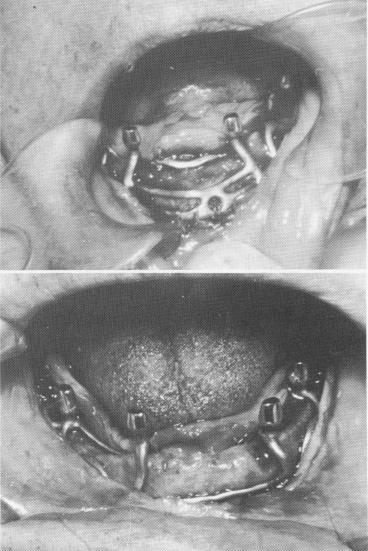
Fig. 12-29. The incision and reflection of the mucoperiosteal tissue, such as is seen in these two different cases, should expose enough of the bone so that the implant can be easily placed into position without pulling and stretching the tissue in those cases where not enough of the bone was exposed.
cised and reflected to allow the implant to be slipped into position. However, postoperative results in this manner are not as good as when larger incisions and reflections are made (Fig. 12-29).
Without generous reflection, the tissue flaps are less mobile and the approximation of their edges is often obtained at the expense of stretching the tissues. Complicating this situation is the fact that the tissues also have to be stretched over the substructure of the implant. By limiting the amount of tissue freed from the bone, less is available for stretching over the implant.
An extremely effective method of dealing with delayed healing by secondary intention has been devised by Metz. He advocates a modified advancement flap technique that avoids many of the problems of reincising the original site. The second surgical phase is performed from 6 weeks to 2 months after the first surgery. At this time the incision be-gins at the point where the distal post will be located. This is easily determined by placing the frame-work in the mouth before the surgery and marking
|
|
Page 544 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|