| Theories and Techniques of Oral Implantology (vol.2) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
Subperiosteal implants 545
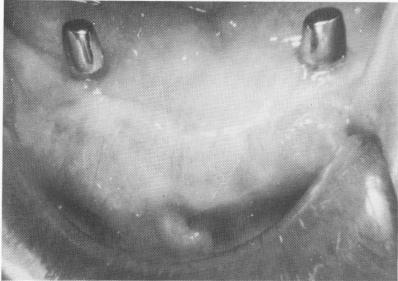
Fig. 12-30. With clean and proper sugery, healing takes place uneventfully. Notice the tissue around the implant posts as they appeared 12 years postoperatively.
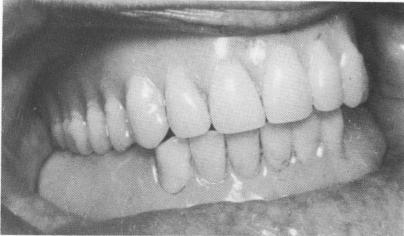
Fig. 12-31. A temporary acrylic stent obtained from a surgical bone bite is fabricated.
the soft tissue with an explorer. To ensure room for the small 7-mm. set screws that might be needed to hold the implant in place, the incision can be ex-tended about 5 mm. posteriorly across the retromolar pads to give sufficient access. The entire incision, however, is made in the buccal and labial mucosa and carried deep enough to assure adequate blood supply. It is not made along the crest of the ridge, as was done during the first surgical phase. Since the incision involves cutting a portion of the buccinator and mentalis muscles, care must be taken not to carry the incision too deeply or the proximal portion of the muscles will have a reduced blood supply.
After careful separation of the mucoperiosteal tissue from the bone and flapping it lingually to expose the ridge, two very small holes are made in the mucosa to allow for the protrusion of the anterior abutments. By this method Metz avoids the entire avascular area resulting from the first operation. As a result healing of the previously intact, highly vascularized buccal and labial mucosa is rapid, occurring in about 3 days. The sutures should not be removed for at least 6 days to ensure adequate fibroblastic proliferation to hold the wound closed.
The flexibility of this outer tissue flap reduces problems in wound closure. However, the main complication in this technique is incising too deeply. This may result in cutting away some of the blood supply to the mentalis or buccinator muscles, causing sloughing of some portions of these muscles.
Although Metz's approach and those of some other operators are useful, Linkow believes that clean, aseptic, and intelligent surgery over the original in-
cision causes a minimum amount of trauma and healing is quite good (Fig. 12-30) .
Setting the temporary denture over the implant
Immediately after the tissue has been sutured, the original or a new prefabricated temporary denture should be fitted over the four abutments. If an old denture is used, its tissue side should be completely hollowed out with a heatless stone or a vulcanite bur so that it can fit directly over the four protruding implant abutment posts without interfering with occlusion.
If a new denture is made, it need only have six anterior acrylic teeth and two posterior acrylic occlusal tables (Fig. 12-31) . No matter which denture is used, it should be tried in the mouth and balanced. The denture should not be in premature occlusion; the bite should not be beyond the original vertical dimension. Fast-setting acrylic should be mixed and placed inside the denture, which is then placed into its proper position over the four implant abutments, and the patient is asked to bite into centric occlusion.
It is imperative to remove the denture long be-fore the acrylic sets, because excess acrylic can slip underneath the abutments to the narrower undercut necks and prevent removal of the denture. There-fore a good procedure is to take the denture on and off every 20 seconds or so as the acrylic sets. As soon as the acrylic starts to get hard, the denture should be left outside the mouth. All excess acrylic inside the post areas of the denture should then be removed so that no undercuts exist. Sometimes, too, a soft denture reliner is used if the operator deems it necessary. It is advisable to slightly hollow out the post
|
|
Page 545 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|