| Theories and Techniques of Oral Implantology (vol.2) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
Subperiosteal implants 543
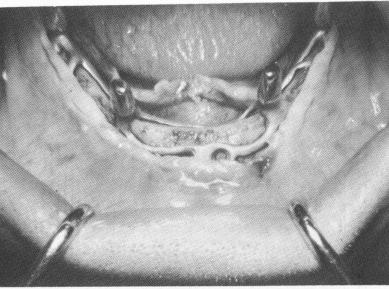
Fig. 12-24. The implant must fit over the bone with 100% accuracy.
Fig. 12-25. Sometimes one to three small set screws are used to stabilize the implant to the bone.
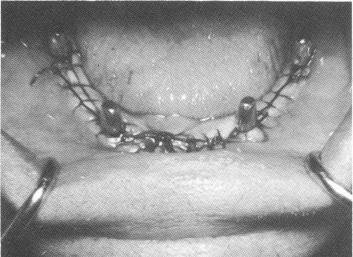
Fig. 12-26. The suturing must adequately close the entire tissue wound and closely adapt the tissue to the four protruding posts.
only establish primary retention; the real security develops as fibromucosal tissue binds itself in and around the meshwork of the substructure.
The holes for the screws are located in the parts of the implant that will cover the densest bone: both external oblique ridges posteriorly and the symphysis anteriorly (Fig. 12-25). Before each screw is set, a small hole is made with a No. 556 fissure bur at right angles to the surface of the bone. While inserting the screws the operator must make sure that they are going in exactly the same direction as the walls surrounding them. Otherwise the screws can create a degree of torque that will either distort the implant itself or interfere with its accurate fit and cause rapid bone resorption. Once the tissues over-lying the implant have healed, the screws can be re-moved, if desired, but this is not necessary. A special Vitallium screwdriver is sometimes used for this procedure.
Suturing the tissues over the implant
One of the most critical steps is the suturing of the tissues to cover the entire substructure of the
Fig. 12-27. An intraoral bandage is festooned and placed over the four protruding posts and over the sutures.
implant. Various thicknesses of silk ligatures are available. Wound closure with atraumatic 000 silk sutures has been the most popular.
Suturing is a time-consuming procedure, and experience has shown that the more sutures, the better (Fig. 12-26). Purse-string sutures are first placed closely around each protruding neck, making sure that the tissue closely adapts to the necks. Second, at least fifteen to twenty interrupted surgical ties should be placed through the approximating edges of the tissue between the posts or necks. Third, any tissue that seems to resist closure should be augmented with a few mattress sutures. An intraoral bandage is again fabricated to cover the sutures and soft tissues (Fig. 12-27), and the patient is dismissed with a head bandage of ice (Fig. 12-28) . It is not imperative to include the intraoral bandage as a routine procedure.
Healing
There is often a considerable difference in the rate of wound healing between the first and second surgical stages. The primary surgery is on mucosal


|
|
Page 543 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|