| Theories and Techniques of Oral Implantology (vol.2) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
542 Theories and techniques of oral implantology
of lower dentures on hand. As long as the teeth are acrylic, which causes less trauma, and not porcelain, the denture can easily be utilized as a temporary splint. Before any actual work is done, the dentist should choose the denture and reline it with a good soft tissue conditioner. When placed over the wound, it should be checked for proper occlusion and any high spots ground away. At this stage, if the patient does not have a denture it is usually not necessary to make one.
Postoperative treatment
The patient should be shown how to keep the wound clean and aid healing after a surgical procedure. On the first day, sterile saline packs should be changed about every 15 minutes for at least 5 or 6 hours. Icepacks should be used to reduce pain and swelling. One should be applied to the jaw for 1 or 2 hours, 15 minutes on the jaw and 15 minutes off. An analgesic, such as 30 mg. codeine phosphate, may be taken every 4 hours for pain.
On the second day, and continuing until the sutures are removed, warm saline solutions should be used to rinse the mouth. At first the solution should be swished gently around the mouth; later this should be more vigorous.
Following-up the first surgical visit
Approximately 7 days later the sutures may be removed. A 3- to 6-week waiting period is then necessary to ensure complete healing. This healing period is essential if the subperiosteal implant can-not be fabricated the very same day the impression is taken. If an attempt is made to insert the implant before the tissues have completely healed, the case could fail because the sutures probably would not hold and the implant substructure will be exposed. This point cannot be emphasized strongly enough; it is exceedingly difficult to make the tissues grow again over an exposed implant.
The Americans Cranin, Weber, and Lew and the Frenchman Audoire claim to have excellent results with a one-stage intervention procedure, which, of course, means two surgical stages within a few hours. Their approach takes about 8 hours. Early in the morning, the first surgical procedure for making an impression is accomplished, the impression is rushed to the laboratory for waxing, casting, and polishing, and then rushed back to the dentist for insertion. The wound is not sutured closed but has barely had time to begin healing. As a result the tissues are easy to reflect. There are two disadvantages to this
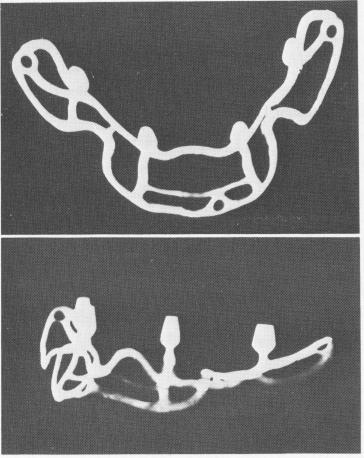
Fig. 12-23. The subperiosteal implants should always be radiographed with special x-ray equipment to be certain that no flaws exist, as they do here.
method: the lengthy day and delay that must be endured by both patient and dentist, and the fact that there isn't enough time to x-ray the substructure for flaws in the metal framework (Fig. 12-23). This is a simple and essential step to avoid using a weak implant that will probably cause trouble later.
Inserting the implant
Another bilateral inferior alveolar nerve block is given, and the original incision line is carefully duplicated with a scalpel. This line is still evident after a 6-week lapse. When reflecting the tissue away from the incision, much less resistance is encountered because the periosteum, which was separated from the bone during the first surgical visit, has not had adequate time to tenaciously rebind to the bone.
The implant is taken directly out of the autoclave and placed into the cold sterilizing solution. The sterilized implant, with the superstructure fitted over the substructure, is then inserted over the exposed bone just cleansed with warm saline solution. The accuracy of the implant's fit can be determined by the close adaptation of the substructure to the important anatomic landmarks (Fig. 12-24). When the implant has been properly seated, the superstructure is re-moved. If the implant is very tight, the overlying tissues can be sutured over it. However, if the fit is slightly loose because of the flat anatomy of the bone, one to three small Vitallium screws 5 to 7 mm. long can be used to hold down the implant. These screws
|
|
Page 542 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|