| Theories and Techniques of Oral Implantology (vol.2) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
536 Theories and techniques of oral implantology
However, Linkow now uses Imput,* a relatively new impression material that handles much easier than the acrylic resin. The heavy mix of Imput is used for making the tray and the light material is used for final accuracy of the bone anatomy.
Exposing the bone
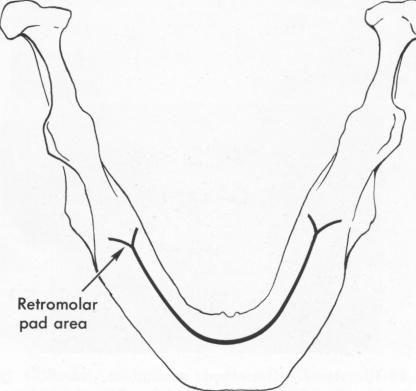
To get an accurate impression of the bone, the soft tissues must be reflected. An incision is made along the crest of the edentulous ridge from one retromolar pad area to the other, making sure that the incision is clear and right down to the bone (Fig. 12-10) . To help avoid stretching and tearing the tissues during reflection, a secondary buccolingual incision is made across the crest-line incision in the symphysis area. Secondary incisions are also made in the retromolar pad areas, but these are not single straight buccolingual cuts. A straight cut can cause a great deal of postoperative swelling and pain. Instead, a very acute V-shaped incision is made from the original incision, with the apex of the V directly in front of the retromolar pad and its legs flanking the pad area buccally and lingually (Fig. 12-11).
With a blunt instrument, such as a periosteal elevator, the soft tissues are reflected downward toward the cheeks and lips and toward the floor of the mouth, exposing the entire mandible. The lingually reflected
*Manufactured by Vicon Products Corp., Mamaroneck, N. Y.
Fig. 12-11. A V-shaped incision was made directly in front of the retromolar pad areas. The reason for this was to pre-vent excessive pain, which often occurs when the incision extends beyond this area.
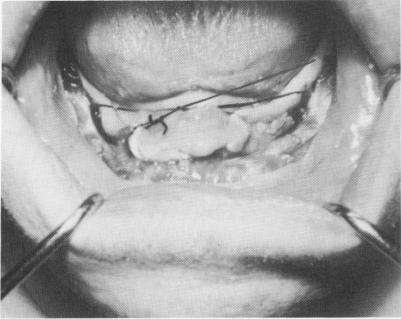
tissues should be sutured so that the tongue is kept in the posterior portion of the mouth and does not interfere with the impression. This is done by simply suturing the posterior aspect of the tissue on one side with the more anterior tissue on the opposite side of the arch, and vice versa (Fig. 12-12). The
Fig. 12-12. The lingual tissue was sutured from one side to the other in a criss-cross fashion to lock the tongue away from the exposed bone so that it would not interfere with the impression, and to keep the lingual tissue away from the bone for more access of the surgical tray, so that it would fit directly over the bone for the impression.
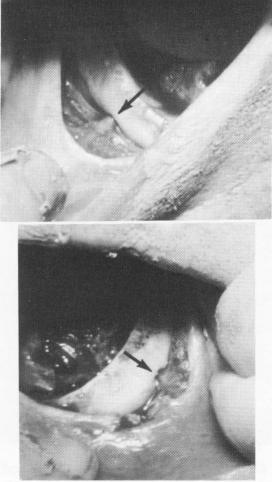
Fig. 12-13. The mental foramina on both sides of the mandible with their exiting neurovascular bundles (arrows) must always be exposed prior to the elastic bone impression.
|
|
Page 536 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|