| Theories and Techniques of Oral Implantology (vol.2) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
Subperiosteal implants 535
the true landscape of the jaw. To do this, a bilateral inferior alveolar block and vertical block anesthesia, produced with 2% lidocaine and epinephrine 1:100,000 is first given the patient. Also injected muscularly is 2 ml. dexamethasone sodium phosphate,* an adrenocortical hormone preparation to reduce swelling. Cold cure acrylic is mixed until it is of a clay-like consistency, then it is molded to the exposed jaw, spraying cold water on it all the time to prevent burning (Fig. 12-8). The resulting tray fits quite accurately and is not overextended, as are trays fabricated in the usual manner. The tray is removed, trimmed, and punched to retain the rub-
*Merck, Sharp and Dohme, West Point, Pa.
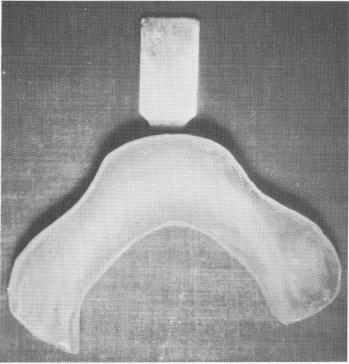
Fig. 12-7. An acrylic tray fabricated from a stone cast that has been reduced in size to assimilate the shape of the under-lying bone. The stone cast had previously been poured into an alginate impression taken of the entire mandible over the soft tissue.
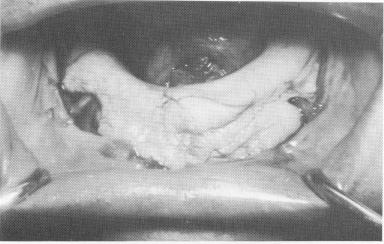
Fig. 12-8. A cold cure acrylic tray is molded directly to the exposed bone (Linkow) and removed before the heat sets in. Note the relief areas on both sides allowing for freedom of the neurovascular bundles that exit the mental foramina.
ber base material (Fig. 12-9). The only disadvantage of this technique is the possibility of the acrylic's burning the soft tissues. This can happen if most of the liquid has not evaporated before the acrylic is placed in the mouth or if the acrylic is allowed to completely set in the mouth without being cooled by water.
Fig. 12-9. The acrylic tray was trimmed and "punched" with many tiny holes (made with a round bur in a contra-angle) and then painted with one of the rubber adhesives, so that it could retain the rubber impression.
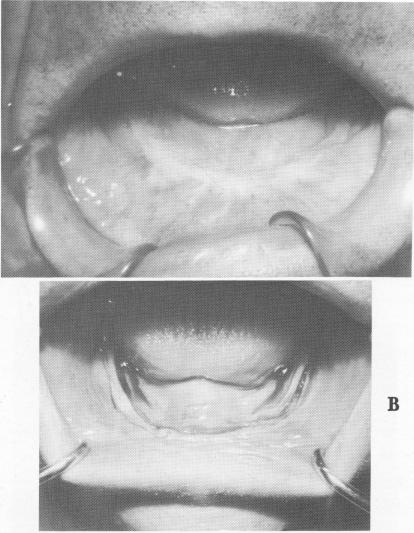
Fig. 12-10. A, The resorbed edentulous mandible just prior to the first surgical stage incision. Note how flat the ridge is when covered by the soft tissue. B, An incision was made along the crest of the soft tissue ridge directly down to the bone. It extended close to the retromolar pad areas on both sides.
A

|
|
Page 535 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|