| Theories and Techniques of Oral Implantology (vol.2) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
A
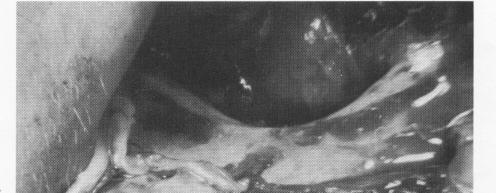
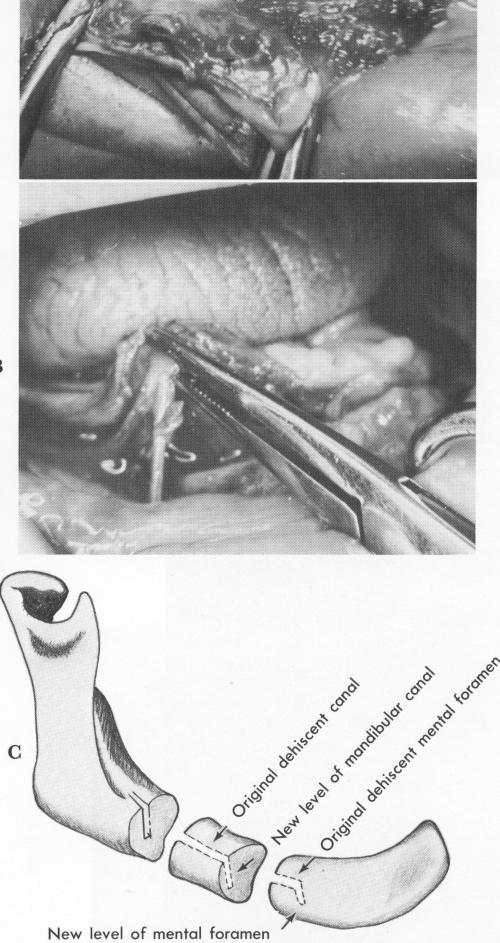
Fig. 12-14. A, The mandible has resorbed to such an ex-tent that the mental foramen is dehiscent at the residual crest. B, Resorption of this mandible left the entire mandibular canal dehiscent. The inferior alveolar nerve is seen being held with a hemostat. C, A dehiscent mandibular canal or mental foramen can be lowered and the neurovascular bundle pushed down into it, enabling a subperiosteal implant to be placed directly over the canal with no nerve impingement.
Subperiosteal implants 537
genial tubercles should be clearly evident in the anterior lingual aspect of the jaw. The mylohyoid ridges should be seen posteriorly, because the lingual extension of the implant will end there and not go below them. Posteriorly, on both buccal aspects, the external oblique ridges should be exposed for the impression, while the entire symphysis should be ex-posed in the anterior inferior labial portion of the mandible.
While reflecting the tissue on both buccal aspects, the operator must be exceptionally careful not to sever or injure the neurovascular bundles of nerves and blood vessels in the areas of both mental foramina. The overlying tissue should be carefully pushed downward with a blunt instrument until a semi-crescent fan-shaped area of tissue appears. This flanks the superior wall of the mental foramen. The bundle should then be more carefully separated, ex-posing more of it as well as the foramen, by pushing the fan-shaped area downward (Fig. 12-13). This should be judiciously executed prior to all impression-taking. It is necessary to exactly locate these anatomic landmarks so that every available surface of bone lying above and near them can be utilized without impinging on them. Sometimes the mandible has atrophied so much that the entire mandibular canal is dehiscent (Fig. 12-14, A and B). For such conditions, Linkow has developed a technique for lifting up the exposed mandibular nerve while lowering the floor of the mandibular canal and mental foramina at the same time with a No. 6 round bur. The nerve bundle is then gently placed back into the revised canal and pushed further into it. Since a new foramen is created, there should be no impingement from the new restoration that will be fabricated for the patient (Fig. 12-14, C) .
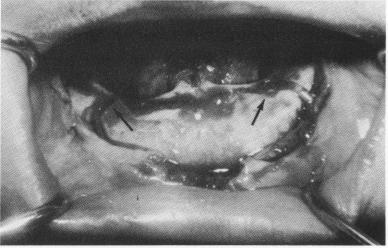
Fig. 12-15. Another case showing the neurovascular bundle of nerves exiting the mental foramina, which are both dehiscent. Arrows point to the areas of the dehiscent foramina.
|
|
Page 537 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|