| Theories and Techniques of Oral Implantology (vol.2) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
Subperiosteal implants 533
Fig. 12-3. The superstructure framework processed inside the implant denture. The tissue-bearing surface of the denture must never touch the soft tissue. In this case it is supported by the four protruding posts extending above the fibromucosal tissue. (From Linkow, L. I.: Re-evaluation of mandibular unilateral subperiosteal implants: a 12 year report, J. Prosth. Dent. 17:509-514, 1967.)
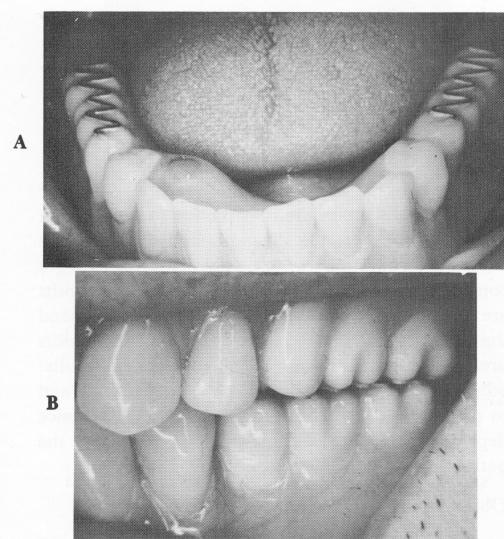
Fig. 12-4. A, Specially designed M.O. (metal occlusal) (Hardy) posterior teeth that consist of metal "rails" em-bedded inside the acrylic teeth for easier cutting of food for those patients who have trouble chewing. B, The superstructure implant denture in the mouth and occluded with the upper denture.
traindicated. It must be realized that since the subperiosteal implant only rests on the bone, it cannot stimulate osteogenesis. Therefore, resorption underneath it could occur if the implant were placed in a mouth with opposing natural teeth.
A thorough medical history must be taken. The history should include all those considerations extensively discussed in Chapter 6. Particularly important for a subperiosteal candidate are blood tests to determine coagulation time and any condition, such as diabetes mellitus, that might hinder healing. Alcoholics are also a poor risk as they seem to have a very slow healing potential. Unless a diabetic patient has a well-controlled condition and must have the implant in order to chew better, avoid the case. It is always a good policy for the dentist to talk directly to the patient's physician prior to implant intervention.
The site should be evaluated before surgery with radiographs. Intraoral radiographs alone should not be the determining factor for exposing any existing pathology. Lateral plate, lateral head, profile, cross-sectionals, topographics, posteroanterior, and cephalometeric and pantographic roentgenograms must very often be used for proper diagnosis.
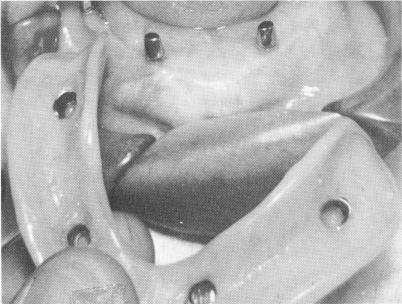
Fig. 12-5. Although this lower subperiosteal implant has been successfully functioning in the mouth opposing a full complement of upper teeth for more than 5 years, such an implant is usually contraindicated in these situations.

|
|
Page 533 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|