| Theories and Techniques of Oral Implantology (vol.2) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
532 Theories and techniques of oral implantology
joined together with a connecting bar. The super-structure becomes an integral part of the implant denture (Fig. 12-3) and "floats" it above the jaw. No portion of the tissue side of the denture should be tissue-bearing.
The implant denture should have acrylic teeth. If the patient has an existing upper denture with porcelain teeth, either make a new denture or change the teeth for acrylic ones Sometimes a patient may
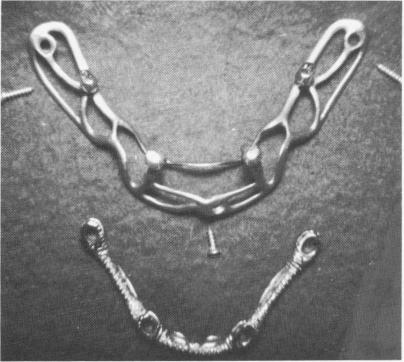
Fig. 12-1. The substructure of the subperiosteal implant is seen on top with three small set screws for primary fixation of the implant to the bone, if desired. On the bottom is seen the superstructure onto which the implant denture is processed.
complain that his implant teeth are too flat, making it difficult for him to chew. The complaint may be alleviated by the use of Hardy Mo-posteriors, specially designed posterior teeth with sharp metal occlusals (Fig. 12-4).
EVALUATING THE CANDIDATE
A mandibular subperiosteal implant should be attempted only when a conventional lower denture has repeatedly proved unsuccessful. If the failure of the conventional denture cannot be overcome by another conventional denture of a better design and fit, the implantologist should carefully evaluate the situation, checking the patient's ridge with its muscle attachments, tissue tonus, height, and thickness, as well as what exists in the opposite arch, whether it be a denture or a full complement of natural teeth. As a routine procedure a full mandibular subperiosteal implant should never be used in the mouth of a patient who has his own full complement of teeth in the opposing jaw. Although such a case may succeed occasionally (Fig. 12-5) , the trauma usually caused by natural teeth could lead to implant failure. Patients with knife-edge ridges are unsuitable candidates unless the ridge is flattened surgically; then at least 6 months to 1 year should elapse before implantation.
While endosseous blade-type implants can function normally against a full complement of opposing natural teeth, a subperiosteal implant is usually con-
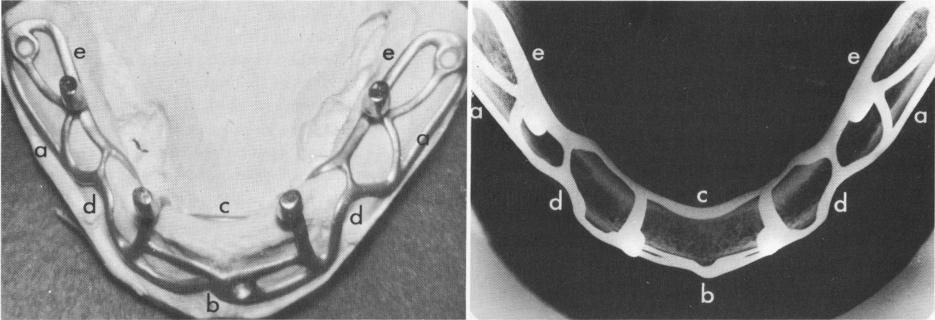
Fig. 12-2. The substructure as it appears on the master stone cast taken from a Neoplex (rubber base) impression of the exposed mandible and in an occlusal x-ray. The peripheral borders of the implant should include the external oblique ridges (a), the symphysis (6), and the genial tubercles (c). The implant should circumvent the neurovascular bundles exiting the mental foramina (d) and extend to, but not below, the mylohyoid ridges (e). (From Linkow, L. I.: Re-evaluation of mandibular unilateral subperiosteal implants: a 12 year report, J. Prosth. Dent. 17:509-514, 1967.)
|
|
Page 532 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|