| Theories and Techniques of Oral Implantology (vol.1) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
144 Theories and techniques of oral implantology
away from the surface of the body, it cannot be successful as a dental implant.
Most dental implant designs extend from the bone, through soft tissues, and into the mouth. This is a potentially dangerous situation in that open pathways for infection are created. The more the soft tissue that invaginates, the greater the pathway. It is therefore important to model a design that hinders the invagination of soft tissue. In Dag's de-sign the large impact area near the surface of the bone invites invagination by discouraging the re-growth of healthy bone. One of the most effective means of preventing soft tissue invagination is to design the implant so that occlusal stresses are directed down into the implant. Dag's design does not incorporate such a feature.
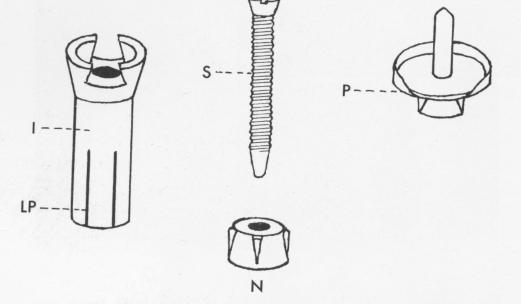
Fig. 5-12. Leger-Dorez's four-piece implant. Insterting the screw (S) with the neckpiece (N) already in place into the shaft (I) causes the lower portion (LP) to flare and brace the implant against the bone. The abutment post portion (P) was then fitted in place to bear the restoration. (From Chercheve, R.: Les implants endo-osseux, Paris, 1962, Librairie Maloint.)
Fig. 5-13. Lehman's arch implant, with its band forming a narrow ellipse. The ellipse can be widened by moving the small rings (or bolts) farther apart on the threaded post.
Leger-Dorez's implant, an early design, consists of four parts (Fig. 5-12) . The shaft was buried in bone with its broad uppermost portion resting near the alveolar crest. The shaft had internal threads to receive a screw fastening a neck into the shaft. As the screw was inserted in the shaft, the lower-most part of the shaft flared. Once the neck was in place, another closely interlocking part bearing the post for a prosthesis was fitted into place.
In spite of the careful engineering of the design and its integral parts, the implant was bound to fail. The broader part of the implant is proximal to the surface of the alveolar crest, an invitation to the invagination of soft tissues and consequent failure. Also, because of the wide diameter of the superficial parts, the impact area near the surface was dangerously large. As for the post itself, there is no surface modulation along the sides of the implant, which is now known to be essential in helping to retain the implant in bone. The pressure from the flaring of the lower portion endangered perforating the cortical plates of bone in a narrow site and probably caused additional bone resorption.
The tantalum arch implant of J. Lehman is a good example of success depending upon both the design and the operative procedure necessary for implantation. The implant consists of a narrow post bearing a band 1 mm. wide and held in place by rings (Fig. 5-13). The band can be shaped to an ellipse of any degree by screwing either or both rings toward or away from the center of the post. The implant is very narrow, which makes it suitable for narrow ridges, and its flaring band makes it adapt-able to open sockets, where the ring can be shaped to fit the socket. The implant was specifically indicated to replace recently extracted teeth or for one abutment post for bridges of average range.
The operative procedure for implanting Lehman's design is rather complex. Although in the hands of a skilled operator some degree of success is possible, the fact that the implant must be set with absolute accuracy is a disadvantage. To set the implant, the mucosal tissues are incised and laid back to expose the bone. Then a slit large enough to suit the flaring band is created. Lehman created his slit by boring two holes at either extremity of the intended site with a cylindrical bur. With the same instrument he gradually defined and deepened the site. This is truly an instrumentation problem that cannot be separated from the implant's design in evaluating the implant. The gradual creation of a slit in a narrow ridge using a cylindrical bore is quite tricky. The

|
|
Page 144 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|