| Theories and Techniques of Oral Implantology (vol.1) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
156 Theories and techniques of oral implantology
the concept is to set into bone a spiraled spring wire and immediately screw into this a shaft portion that would bear the prosthesis. As the shaft portion is inserted, the spring expands slightly, making the implant quite snug. Whether or not the implant is successful depends on the shape of the spring, the number of spirals, and the distance between the spirals.
In the coil, or spring, implant of George Trattner, seen on the left in Fig. 5-39, there is little space through which hone can grow between the coils. Therefore, although the implant is tight when first inserted, it tends to loosen as bone resorbs and fibromucosal, not bony, tissues replace it. Isaiah Lew's variation, shown in the center, differs in that he added more coils and a collar. This latter increases the impact area, an undesirable addition.
In the coil-vent of Leonard Linkow, shown on the right in Fig. 5-39, the spirals are more widely spaced, providing room for bone regeneration. Also, because the implant post is vented or contains a window, there is more room for freer circulation of blood- and bone-rebuilding elements. Although the idea appears valuable, there are several flaws. The coils or springs are too large for many sites, and the operative procedure is much more difficult than those of other types of equally or more successful implants.
Another implantologist who gradually modified his earlier, partially successful designs into highly successful models is the Italian Giordano Muratori. Muratori's early design, proposed in 1963, consisted
of a spiral encircling two narrow vertical uprights and surmounted by an internally threaded shaft (Fig. 5-40). This latter part was much too bulky and, being the same diameter as the spiral part, invited tissue breakdown and soft tissue invagination. Even with this drawback, success was possible (Fig. 5-41).
By 1967 Muratori greatly reduced the perils of soft tissue invagination by modifying the design of the solid portion of his implant (Fig. 5-42). He made it narrower and rounded it. This new implant, made of titanium, has been highly successful to date.
One of the most successful variations in the spiral-post was proposed by the American, Leonard I. Linkow, who designed the vent-plant in 1963 (Fig. 5-43). Although it was essential to bury the open spirals of the conventional spiral-post well away from the alveolar crest to prevent soft tissue invagination, this could prove to be a disadvantage. Unless the implant were securely settled in its site at the onset of insertion and well stabilized, an unfortunate lever action could result that could destroy surrounding bone. To reduce the dangers of this, Linkow made the spiral portion solid, which kept soft tissues from creeping through the open spirals, and moved the spiral portion closer to the surface. Having closed the spirals, he opened the base with a vent, or window, through which bone could grow. Because bone regenerates at the deepest portions first, it can soon grow through the vent and secure the implant. The generous space at the base permitted by the vent also
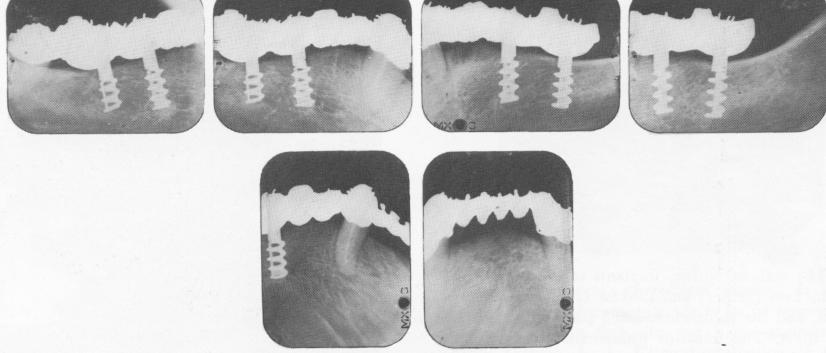
Fig. 5-41. Muratori's early implant inserted by Linkow. Bone regrowth is good, and the x-rays afford a better idea of how the spiral is wound around the vertical struts.
|
|
Page 156 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|