| Theories and Techniques of Oral Implantology (vol.1) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
The evolution of dental implants 159
himself has successfully inserted his own implants, perhaps the operative technique was at fault. What is really puzzling is the relationship of bone to the implant. Whereas other studies indicate the necessity of a connective tissue membrane around an implant, it is difficult to tell whether or not one formed around the coated vent-plant, yet it is successful in this demonstration. It is Linkow's belief that tissue grows through the open vent, acting as a suspensor type ligament. He also believes that the vent-plant should be narrow at the alveolar crest. Further studies of the tissues around nonmetallic implants are currently being investigated.
UNCOMMON ENDOSSEOUS IMPLANTS
Numerous ideas for implants embedded in bone have been developed. Some were practical, based on apparently sound reasoning. Others were highly impractical, primarily because of the difficulty in inserting them. These should be included in any history of dental implants to realistically represent some of the numerous and wide ranging approaches pro-posed to help the partially or totally edentulous patient.
Reexposed implants
Several implantologists independently evolved the apparently logical concept of reexposed implants. To isolate an implant from a septic oral medium, the idea of burying it in the bone and allowing the tissues to heal over it until the implant was secure seemed quite practical. Once the bone had grown around the implant, as determined by radiographs, its uppermost part was to be reexposed and the prosthesis-bearing part of the implant inserted. How-ever, it was misleading to believe that isolation and its resulting benefits could be preserved if the buried implant were to be reexposed. Microbes can invade a site upon its second exposure as well as upon its first. Also, an injured site should have some means of draining. Another disadvantage of the buried implant method is that whereas a functioning implant will restore near-normal condition in the site and pro-mote bone regeneration, a buried implant cannot.
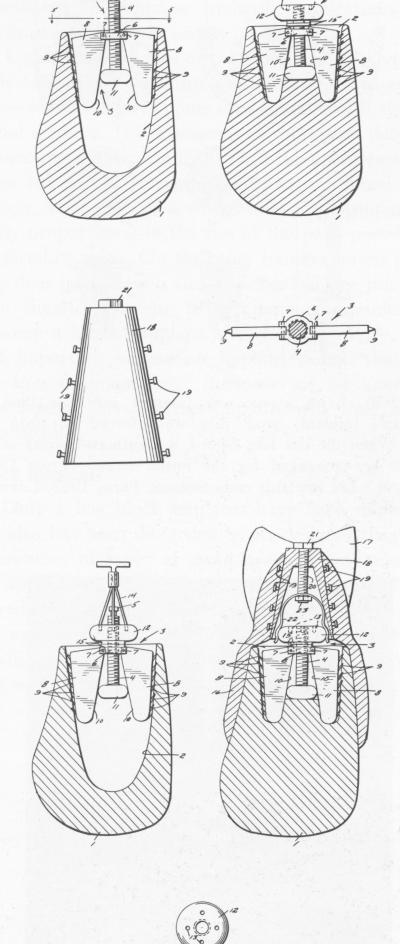
Among the first proponents of the buried implant was the American Glenn D. Irwin.* In 1941 Irwin filed a patent application for an implant to be set in the site of a recent extraction (Fig. 5-49). The flaring sides were to expand and brace the implant in the site, and minute prongs on the edges of the
*Irwin, G. D.: Artificial denture retainer, U. S. Patent Office Serial 2,258,207, filed March 18, 1941.
sites were to grip the bone. Supposedly, once bone had regrown into and around the implant and it was secure, a denture was to be fitted over the protruding post and affixed to it. This would provide a non-movable saddle bearing artificial teeth.
The design carefully provides for minor adjustments to be made in fitting the implant to the site
Fig. 5-49. Irwin planned to set this implant in a recent ex-traction site and, when the site had healed, reexpose it and fasten the prosthesis to it. The sides of the implant with their small extensions were to expand to fill the site and secure the implant.
|
|
Page 159 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|