| Theories and Techniques of Oral Implantology (vol.2) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
650 Theories and techniques of oral implantology
to the bone (Fig. 15-61). During this procedure, radiographs were taken to guide the operator in directing the pins around the sinus (Fig. 15-62). By not suturing the soft tissue covering the area of the root resection, the anterior pin was clinically visible as it traversed the bone void separating the sinus floor from the shortened root (Fig. 15-63) .
The excess was cut off the protruding pins, and the remaining ends were carefully notched with a fissure bur for added retention during their fusion with acrylic. The protruding pins were then fused together with cold cure acrylic, using the brush-on technique (Fig. 15-64). Only a minimum amount of acrylic was used, to avoid interference with the fitting of the superstructure. The superstructure was tried on before the acrylic hardened (Fig. 15-65). This ensured that only a minimum amount of adjustment was necessary when cementing on the superstructure.
The superstructure was then cemented over the template. Oxyphosphate of zinc cement was used
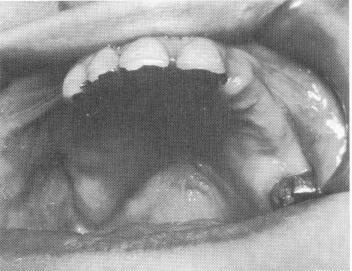
Fig. 15-70. The remaining upper teeth are seen. The alveolar bone in the right posterior quadrant was completely resorbed buccolingually to such an extent that the original ridge crest was so far lingual to the lower ridge that the upper teeth were completely lingual to the lower ones, with no contact.
Fig. 15-71. The five remaining lower teeth.
inside the crown covering the gold post extending from the template, and acrylic was used inside the crown fitting over the acrylic core. When the cement hardened, it was trimmed. Sutures were placed in the area of the apicoectomy (Fig. 15-66). Roentgenograms were taken (Fig. 15-67) .
The sutures covering the area of the apicoectomy were removed a week later. Three weeks later the tissue had completely healed (Fig. 15-68). Eighteen months after surgery, x-rays showed the healed site (Fig. 15-69) .
This case was an unusual approach to providing room for a proper triplant. The fact that the second bicuspid tooth had previous root canal therapy helped the operator decide on an apicoectomy. How-ever, such an approach can become an almost routine procedure if the operator decides it is beneficial to the patient to devitalize a tooth in order to pro-vide a fixed partial denture for a posterior edentulous area. An alternative, and better, approach for such a problem is to insert a blade-vent in the maxillary tuberosity. This involves no devitalization of teeth and gives added security for a fixed partial denture.
Case 6
Using the zygomatic arch as an implant site
There have been unique and uncommon situations in which a patient has no normal type of occlusion and cannot tolerate a removable appliance. In• the following case, the woman had multiple anomalies that made conventional removable dentures impossible.
The patient had five remaining maxillary teeth—the left central incisor, the left second molar, and the right central, lateral, and cuspid teeth (Fig. 15-70). Furthermore, her right maxillary ridge was practically nonexistent; if teeth were constructed to
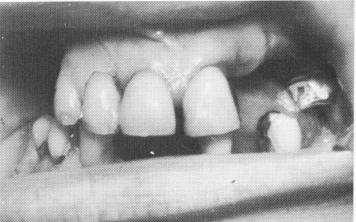
Fig. 15-72. From an anterior view both lower right bicuspids are seen to extend buccally far more than the re-sorbed opposing maxillary ridge.

|
|
Page 650 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|