| Theories and Techniques of Oral Implantology (vol.2) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
Atypical implant situations 645
lateral fixed partial dentures were cemented over the lower abutment teeth (Fig. 15-48) .
As a result of the procedure, the patient's over-jet was greatly reduced and his bite was much improved (Fig. 15-49). The patient no longer had to search for a normal centric relation position be-cause he now automatically retruded to it. The Panorex clearly demonstrates the results (Fig. 15-50).
Case 5
Performing an apicoectomy to create space for an implant
When a post type implant cannot be introduced into the bone in a posterior edentulous maxilla be-cause of a low-flaring sinus, a triplant intervention may be necessary. Three extremely important considerations for the triplant technique are the density of the osseous structure in the area, the depth of bone available, and the anteroposterior extension of the sinus. It is also imperative that there be enough bone in the maxillary tuberosity area for the distal triplant pin or pins. Anteriorly, there must be enough osseous tissue separating the root of the most posterior natural abutment and the floor of the maxillary sinus so that the pin can be inserted with the proper angulation and depth. Unless there is at least 2 mm. separating these two landmarks, a properly executed triplant cannot be performed; thus, such an implant is usually contraindicated. Some-times, however, it is possible to create a space between the floor of the low-hanging maxillary sinus and the apex of the root of the last tooth by reducing the length of the root with an apicoectomy. The following case describes such a procedure.
The patient, a healthy woman in her early fifties, desired a fixed rather than a removable partial denture to replace her missing maxillary molars.
Periapical intraoral radiographs of the maxillary right bicuspid teeth and of the edentulous posterior area were taken, as was a Panorex radiograph. The results disclosed that the anterior extension of the floor of the maxillary sinus was in direct contact with the apex of the root of the upper second bicuspid tooth. The x-rays also revealed that successful root canal therapy had been performed on the second bicuspid tooth.
Upon examining the mouth clinically, the two bicuspid teeth were found to have very short clinical
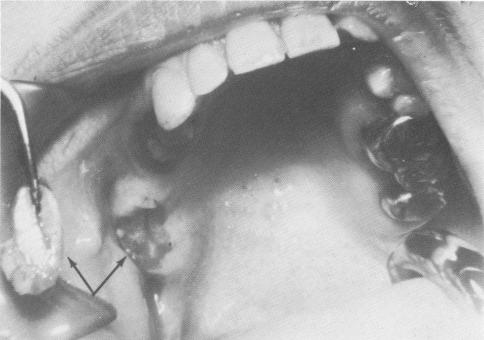
Fig. 15-52. Since there was no interocclusal space between the last lower molar and fibromucosal tissue in the maxilla that existed distal to the cantilevered molar, a large portion of the thickened fibromucosal tissue that was contacting the lower molar was removed surgically (arrows).
Fig. 15-51. The patient could not function any longer with her upper three-unit fixed partial denture using the two bicuspids and a cantilevered molar, which was driven into the fibromucosal tissue, as the abutments.
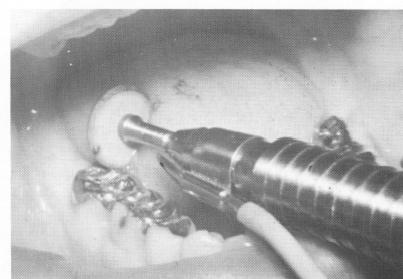
Fig. 15-53. The occlusal surface of the last molar inlay was also reduced.

|
|
Page 645 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|