| Theories and Techniques of Oral Implantology (vol.2) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
636 Theories and techniques of oral implantology
means that the condyles are able to retrude comfortably, and a more correct centric position can be established. In such cases, which are often referred to as false Class III mesiocclusions, the anterior maxillary and mandibular incisors and cuspids can be shortened until posterior contact is produced. However, the approach to such a procedure must be conservative. If the anterior teeth cannot be brought edge-to-edge, grinding alone will not correct the condition. If the underbite is extreme, the
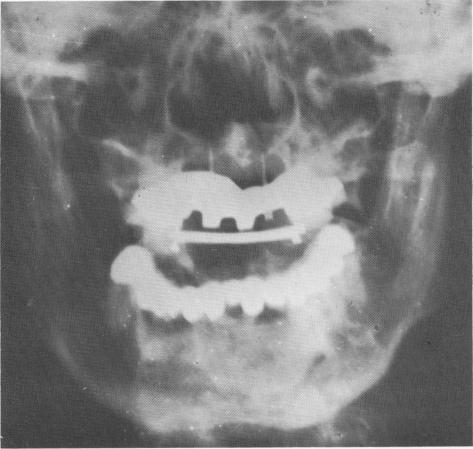
Fig. 15-20. A posteroanterior view of the case showing the full arch lower fixed denture as well as the maxillary anterior narrow ridge implants, template, and bar. The acrylic teeth cannot be noticed on the radiograph.
degree of grinding necessary to establish freeway space will be prohibitive. Therefore grinding by it-self is not indicated. Where occlusal contact of the posterior teeth cannot be achieved, grinding alone should not be attempted. In these instances, if orthodontia is not feasible, prosthetic or surgical procedures should be employed in combination with grinding and occlusal rehabilitation to obtain the desired occlusion.
If posterior contact cannot be obtained by conservative grinding of the anterior teeth, the posterior crowns can be raised to meet the new occlusal heights. All missing teeth should be included in the fixed bridgework, and all malformed, malpositioned, or unattractive teeth in the anterior region should be individually restored with full crown coverage. If, however, posterior contact was attained by anterior grinding, all crown restorations can be constructed at the same occlusal height.
In all bite-raising cases, the freeway space must be carefully determined before any attempt is made to increase the crown lengths of the teeth. At rest position a physiologic freeway space must remain after the bite-raising has been completed; 1 to 2 mm. will suffice.
In this case a 43-year-old male patient appeared to have a severe Class III malocclusion (Fig. 15-22). However, when the mandible was retruded, contact was made between his upper and lower incisors (Fig. 15-23).
Using the incisal contacts as a guide, the patient's upper teeth were prepared, and the laboratory fabricated posterior veneer crown castings and
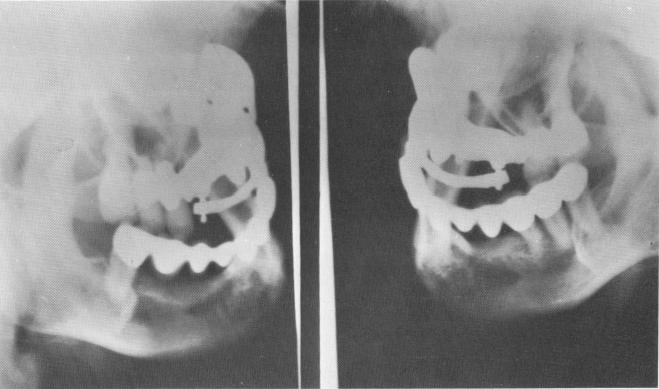
Fig. 15-21. Two lateral plate views.
|
|
Page 636 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|