| Theories and Techniques of Oral Implantology (vol.2) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
Causes of implant failure 615
A
C
A
C
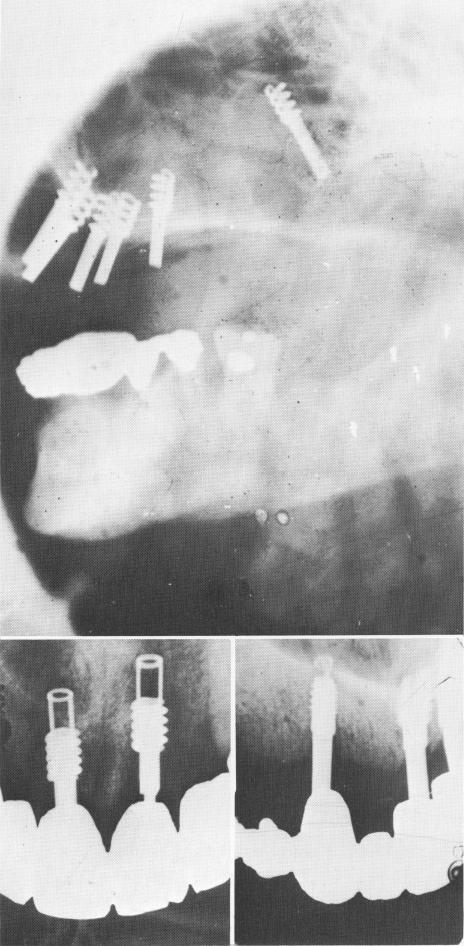
Fig. 14-12. A, A Chercheve type of spiral implant that was pushed into the maxillary sinus. It must be removed as quickly as possible. (From Linkow, L. I.: Alloplastic implants. In Goldman, H. M., Forrest, S. P., Byrd, D. L., and McDonald, R. E.: Current therapy in dentistry, vol. 3, St. Louis, 1968, The C. V. Mosby Co., pp. 335-356.) B and C, Radiographs showing various vent-plants perforating the nasal vestibulum.
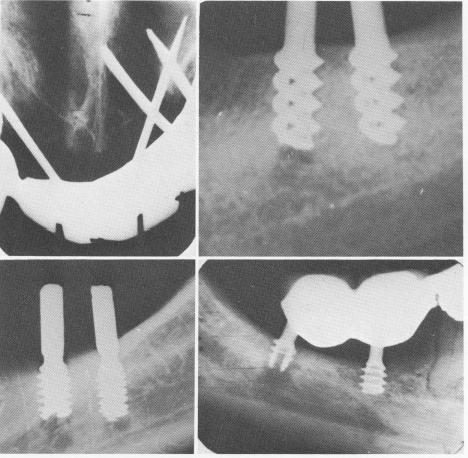
Fig. 14-13. A, Pin implants are deeply embedded in the nasal vestibulum. B, A number of operative mistakes caused failure with the implants. The trephining of bone below the first implant perforated the mandibular canal. Also, the spirals were too close to the alveolar crest. A two- to three-spiraled implant should have been used insted of the four-spiraled one. (Arrow points to area of canal perforation.) C, Both helical burs penetrated the canal, causing temporary paresthesia. However, the most posterior implant was also set into the mandibular canal and had to be removed. D, The posterior implant was not firmly anchored because the underlying bone was overtrephined with the helical bur. In most situations where the canal is involved either by the instrumentation prior to the implant insertion or by the implant itself, a paresthesia is usually the result.
resistance from a spicule of bone and assume that the bottom of the prepared hole has been reached. He thus leaves the implant too high, causing the invagination of epithelial tissue into the spirals.
Setting the implant as deep as the prepared hole is usually a problem only with the spiral-shaft implant, and a number of failures—particularly by a timid, inexperienced operator—may result (Fig. 14-15). The operator should always carefully check his x-rays and review his previous estimates as he seats the implant. When he is sure that the implant has not been set deeply enough and yet he feels resistance, the hole should be widened so that the spiral-post implant can be inserted to its maximum depth. As has been previously mentioned, forcing an implant—particularly a spiral-post implant—into its site may result in the implant's breaking.
There is less chance of incorrectly seating an implant when using the vent-plant or the blade-vent.
B
B
D
|
|
Page 615 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|