| Theories and Techniques of Oral Implantology (vol.2) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
586 Theories and techniques of oral implantology
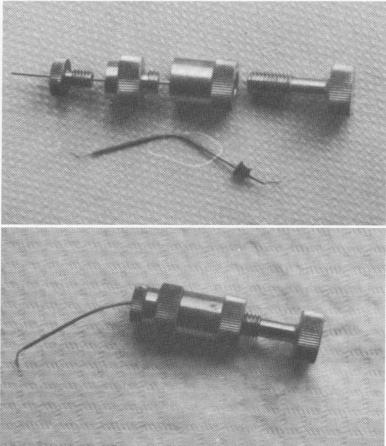
Fig. 13-8. The Morgan (Evamore) paste propelling screw. A, The apparatus disassembled. B, The apparatus assembled, with iodoform (Kri I) paste extruded.
unknown in the United States until recently. In addition to acting as a mechanical barrier to cement, Kri paste also is a good local disinfectant, is resorbable, and can arrest hemorrhage. It is also easy to deposit and, if necessary, remove.
Ledermix paste has been mixed with Kri paste to enhance its antibiotic and anti-inflammatory proper-ties, but the results do not differ from those of using Kri paste alone. As a barrier, Kri paste alone seems best.
To insert the Kri paste to the apex of the tooth, an Evamore (Morgan) paste-propelling screw is recommended (Fig. 13-8). It is, of course, possible to position the paste by other means, such as Lentulo spirals, but the Evamore screw will greatly facilitate the work.
Anesthetics. The kind and amount of anesthetic needed depends upon the site. For front teeth, regional anesthesia is recommended to lessen irritation. For lower premolars and molars, infiltration anesthesia is advisable because it does not dull the main mandibular nerve. Although the danger of injuring this nerve is very slight, it should nevertheless be considered. If the nerve is sensitive, the patient can warn the operator of approaching danger.
Sometimes it may be expedient to instill anesthesia by pressure or to inject a few droplets of anestheticum through the foramen into the periapex of the tooth. Because the bone itself exhibits no pain,
only a few drops for the periapex and the periodontium are needed. Although this technique is deemed dangerous by some dentists, extensive experience with hundreds of cases indicates otherwise.
The usual premedication and postmedication drugs, both anodynes and antibiotics, may be given, although they will rarely be necessary.
OPERATIVE PROCEDURES
Inserting an endodontic implant for tooth stabilization is basically a two-part operation. The first part is an endodontic procedure, which consists of removing the pulp tissue in the canal, sterilizing the canal, and then packing it with the proper filling material. The second phase is the implant procedure, which consists of entering the bone beyond the apex with proper spiral rotary instruments, stopping existing hemorrhages, treating the osseous tissue with antibiotics, and, finally, inserting the endodontic implant with the proper cement.
The step-by-step techniques of creating the site and setting the implant vary slightly from operator to operator. One of the most simple and effective approaches is that of Hans Orlay. Orlay's procedures, diagrammed in Fig. 13-9, are as follows.
First, the root canal is trephined. When sufficient bone is available at the apex of the tooth to hold the pin, the implant will be inserted along the axis of the root canal. This frequently necessitates entering the tooth on the incisal edge or some visible part of the crown, as the rigid endodontic implant usually can-not be bent to follow the curved pattern of the tooth.
Second, the canal is widened following Wlakhoff's method to permit the eventual passage of root canal instruments up to gauge 15. This is done by alternating tapered and cylindrical reamers, sizes 3 or 4. At first the enlarging should stop just short of the apex, which should be protected by Kri paste in order to avoid contamination with debris. During this process the canal should be frequently cleaned and irrigated.
Third, the canal is widened to a 9 or 10 cylindrical bur without piercing the apex. Again Kri paste is used in the apical region as a mechanical barrier.
Fourth, the endodontic pin is inserted to see whether it fits properly. An x-ray is taken to deter-mine how far it extends into the tooth. If the proper depth has been reached, just shy of the apex, the pin is marked. Because the labial and linguopalatal emergence points may differ as much as 3 or 4 mm., marks should be made circumferentially. Now the
A
B
|
|
Page 586 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|