| Theories and Techniques of Oral Implantology (vol.2) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
540 Theories and techniques of oral implantology
The surgical tray, regardless of how it was made, should first be treated with one of the "adhesive" agents that allows the rubber to bind with it.
A rubber base material (Coe) or Neoplex (Surgident Co.) is usually the choice material for the bone impression. When using rubber, it is mixed to an even consistency and then placed into the tray and held in the mouth for at least 10 minutes to set. The advantage of using Neoplex instead of rubber, although both set at about the same time, is that the operator can mold the Neoplex in his hand like clay. He can first mold it over the exposed bone and around the landmarks before setting the tray over it. After the impression has hardened, it is removed and checked for accuracy (Fig. 12-18, A). Some operators take two impressions as a routine procedure. However, one lessens the danger of any impression material slipping underneath the neurovascular bundles or a dehiscent nerve. The less aggravation brought to bear on these structures, the better off the patient is.
Obtaining a bone bite
While the mandible is still exposed, a surgical bone bite using wax should be taken. The wax is merely heated and placed over the exposed bone. The patient closes in a retruded position in centric relation and meshes with the teeth of the opposite arch. This bone bite tells the technician how high to make the four abutment posts that will protrude into the oral cavity.
A more accurate wax bite may be taken with the acrylic tray containing the rubber impression still in the mouth. The resulting bite is more ac-curate because the rubber impression is the exact duplicate of the bony ridge. An alginate impression also must be taken of the opposing jaw.
More recent developments by Linkow include an accurate light-bodied Imput wash inside a heavier Imput body tray. While the impression is still in the mouth, another heavy-bodied Imput mix is placed against the opposing teeth and the patient is guided into centric relation. When the mix sets, it adheres to the tray; the impression of the exposed mandible and interocclusal record of centric relation are accomplished together (Fig. 12-18, B to D) .
An accurate measurement of the soft tissue over-lying the four areas where the abutment posts will protrude should also be taken and sent to the technician. In this manner the height of the necks can be accurately determined. The tissue in the mandible is usually no thicker than 1 to 2 mm. However, if the tissue is not measured accurately and the neck is too long, the prosthesis-bearing post may be made much too short to firmly hold the superstructure. As an example, in one case it was necessary to cast a gold coping to cover the extra long neck so that the foreshortened abutment post could gain retention (Fig. 12-19). Unnecessarily long necks may also cause tension that results in the exposure of the primary strut (Fig. 12-20) . Such a situation may be
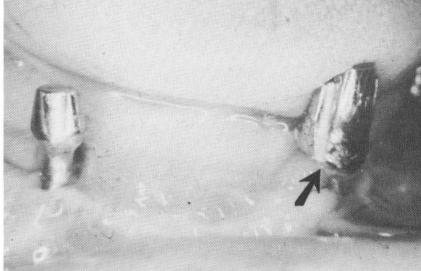
Fig. 12-19. An extended gold coping is sometimes cemented over an improperly designed implant post. In this case too much of the narrow neck below the post was exposed; the neck was made too long at the expense of the fore-shortened post, greatly reducing its retentive qualities. The gold coping restores the anatomy, improving the retention required to hold the implant denture. Note also the excessively long neck and short post on the right side, which was also improperly designed.
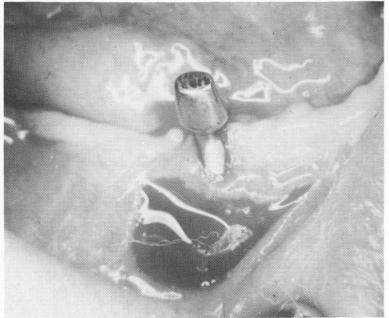
Fig. 12-20. The tissue sometimes recedes around an excessively long neck, especially if a high muscle attachment exists in the area. A relief incision is often made horizontally below the exposed strut and allowed to heal by secondary intention. This reduces the muscle pull, and sometimes the tissue readapts to its original height around the neck.
|
|
Page 540 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|