| Theories and Techniques of Oral Implantology (vol.2) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
Endosseous blade implants 517
drawback was that if there was not enough dense bone, then there could not be sufficient support for a continuous blade implant. Therefore a support was added across the palate to more closely adapt the implant to its site. The implant is called the palatal bar horseshoe blade.
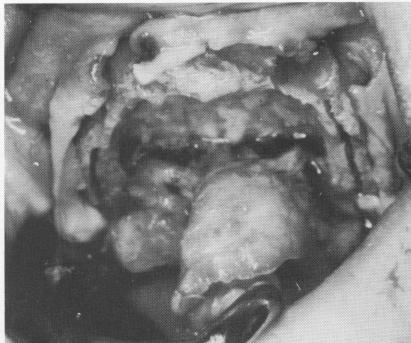
This patient had had recent extractions (Fig. 11-177). The fibromucosal tissue was incised and separated from the bone. Because of the palatal ex-
tensions needed in this new implant design, most of the hard palate was also exposed, including the posterior nasal spine and greater and lesser palatine foramina. The palatal tissue was then retracted in a posterior direction from the incision. Grooves were planned only for those areas where the alveolar crest was wide. In this particular case they were made in the left posterior alveolar ridge, ending anteriorly just distal to the recent open
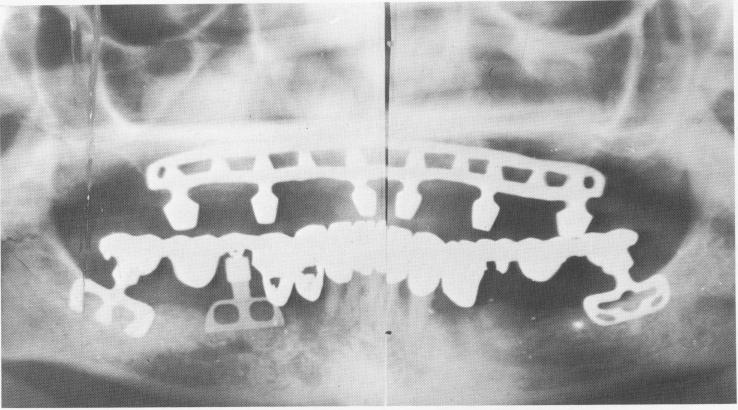
Fig. 11-176. A Panorex of the completed maxillary restoration. The mandibular restoration had been successfully functioning for over a year. Since it was one of the earlier cases the prosthesis was prefabricated before the implants were set into the bone. Large holes were made inside the pontics corresponding to the implants and then they were locked to the protruding posts with acrylic resin, which cannot be seen on a radiograph. This method is no longer done since the blades can remain unsupported for many weeks after their initial insertion. (From Linkow, L. I.: Status of oral implants, 1969, Inform. Odontostomat., Vol. 1, 1969.)
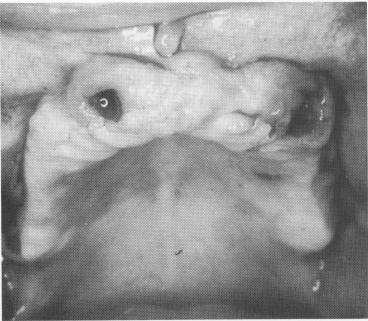
Fig. 11-177. The edentulous maxilla with recent extractions. Note the density and irregularity of the fibromucosa.
Fig. 11-178. The knife-edge ridge was only grooved laterally because the anterior portion flared.
|
|
Page 517 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|