| Theories and Techniques of Oral Implantology (vol.2) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
466 Theories and techniques of oral implantology
(Fig. 11-12). Final cementation occurs, and the occlusion is once again checked and balanced (Fig. 11-13).
In certain situations, such as in a mandible with extremely dense bone, it may be difficult to tap the entire blade into the bone until its shoulders are slightly below the alveolar crest. In order to minimize the trauma caused by hard tapping, the implant should be removed with forceps and the groove sufficiently deepened with the bur. The implant is then replaced and lightly tapped to the desired depth. In such situations, as soon as the experienced operator gets the feel of the bone, he will immediately drill about 5 or 6 mm. deep to avoid removing and re-placing the blade. Generally the depth of the groove is proportional to the density of the underlying cancellous hone. The denser the bone, the deeper the slit. However, Linkow firmly suggests that the groove always be made the same depth as the blade portion' of the implant to be used, or even deeper.
If a blade implant is not absolutely firm after its final placement, it should be removed and re-placed with a thicker implant. Careful evaluation will determine whether the second implant should be different in design, with a longer as well as a thicker body. If a longer implant is desirable, the groove must first be lengthened to fit the new blade. A loose implant should always be substituted. Besides being undesirable for healing reasons, it will cause pain and discomfort.
If either shoulder does not seat evenly so as to
maintain the post of the implant in a vertical position and parallel to other abutments, either the implant can be removed or the protruding post can be prepared with a tapering diamond stone to make it parallel to the other abutments. The offending area should be slightly deepened with a No. 700L tapering fissure bur until the blade can be seated properly.
Simple interrupted sutures should be used to approximate the incised tissues. Mattress sutures are not necessary, as they are around the posts of subperiosteal implants, because healing over the blade implant is usually rapid and uneventful.
When a blade is contemplated around the curvature of an arch, such as in a cuspid area, the trench or groove must be curved to follow the center of the ridge. Before the blade implant is inserted, it must be bent to exactly fit the curved groove; other-wise, it could fracture or break off a piece of the surrounding bone as it is tapped into place.
Advantages
The blade implant has a number of distinct ad-vantages, both in design and in insertion.
1. It offers far more resistance to lateral and occlusal forces than any other types of endosseous implants. This is because the body of the blade intimately contacts more alveolar bone than does a screw or pin type implant. Purely from a mechanical point of view, the average blade contacts more bone than does a large three-rooted molar. This can play
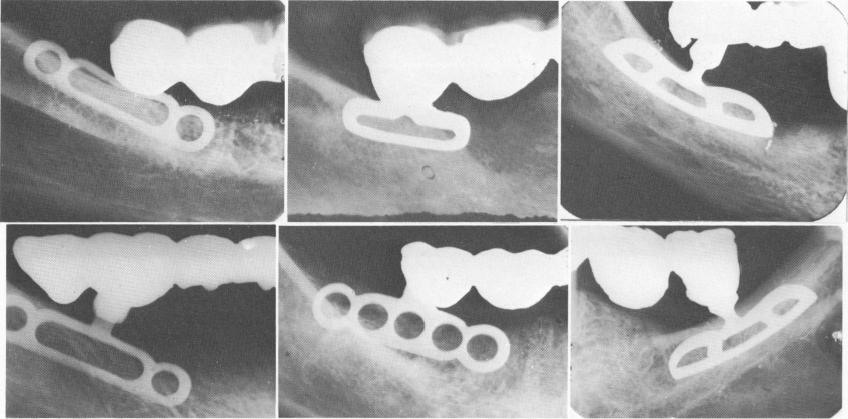
Fig. 11-15. Blades for shallow areas. (From Linkow, L. I.: The endosseous blade, a new dimension in oral implantology, Rev. Trim. Implant., Nov., 1968.)
|
|
Page 466 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|