| Theories and Techniques of Oral Implantology (vol.1) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
100 Theories and techniques of oral implantology
Linkow on vent-plants
Case 1. This opportunity for obtaining bone blocks for histologic examination came about through an error in judgment. The error: endosseous implants should not have been used. After little more than 5 months, a full arch maxillary fixed denture had to be removed with all of its implants.
The patient was referred because he could not wear a conventional full upper denture. He previously had been fitted with four or five well-made, removable dentures, and he now wanted a fixed prosthesis. Initial radiologic interpretation should have been enough evidence to contraindicate implants. The floor of the sinus was extremely low and extended anteriorly to the cuspid teeth, making it impossible to insert vertical post implants posteriorly. (At that time, some years ago, there was little choice of implant design. Today the blade implant can be used.)
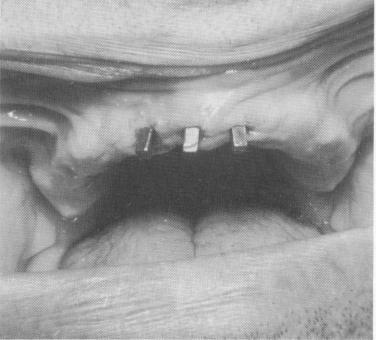
Three vent-plants were placed in the anterior quadrant: one in each lateral incisor region, and one in the nasal septum (Fig. 4-33). A full-arch scalloped template—with a posterior palatal bar—was cast to fit passively over the soft tissue covering the crest of the alveolar ridge. Anteriorly the template contained three copings that fitted over the protruding shafts of the vent-plants.
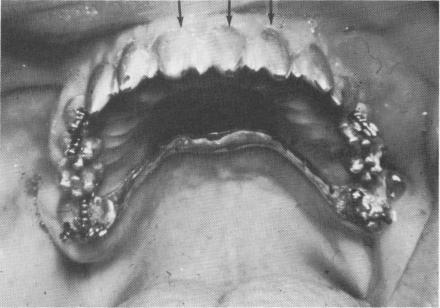
The template was cemented into position with hard cement placed inside the three anterior copings. Pin implants were driven through predetermined holes in the posterior extensions of the template and extended into the underlying alveolar bone to avoid the low-flaring maxillary sinus (Fig. 4-34). The pins were fused together in a series of three each with cold cure acrylic. The acrylic-covered pins were then prepared to form abutments (Fig. 4-35) . A full-arch acrylic-over-gold fixed denture was then fabricated and cemented over the template containing the three anterior gold cores and six acrylic cores.
After 3 months the template loosened and the patient complained of pain on mastication. For an-other 2 months it became progressively looser. To possibly save the prosthesis by immobilizing it, two tantalum pin implants were obliquely driven through the posterior palatal connecting bar, which was in passive contact with the tissues, to end in the buccal plates of bone (Fig. 4-36). The pins were then bent flush to the palatal bar, notched for better retention, and fused with acrylic to the palatal connecting bar, which was also notched (Fig. 4-37) .
Fig. 4-33. Clinical view of the anterior vent-plants.
Fig. 4-34. Pin implants were used posteriorly to avoid the maxillary sinus. Arrows point to copings covering vent-plants.
Fig. 4-35. The acrylic cores fusing the triplant pins were prepared as posterior abutments.

|
|
Page 100 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|