| Theories and Techniques of Oral Implantology (vol.1) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
The evolution of dental implants 137
in the great majority of cases. By tracing the evolution of the endosseous implant, the reader will develop an appreciation of why these implants are successful and learn to anticipate some of the problems in evaluating a site and choosing the type of implant best suited to it.
POST TYPE ENDOSSEOUS IMPLANTS
Historically, designs for endosseous implants began with the rather naive assumption that an implant that closely resembled the natural root or roots of a tooth should work best. Therefore some of the first designs were basically posts modified to resemble natural roots. However, what anchored the natural root to its site—the close relationship between the surrounding bone and the root established by Sharpey's fibers was absent in the implant. It was quickly recognized from failures that an implant must in-corporate some additional, artificial retentive devices.
One of the earliest endosseous implants, and a surprisingly good one too, was that of Edwin J. Greenfield of Wichita, Kansas.
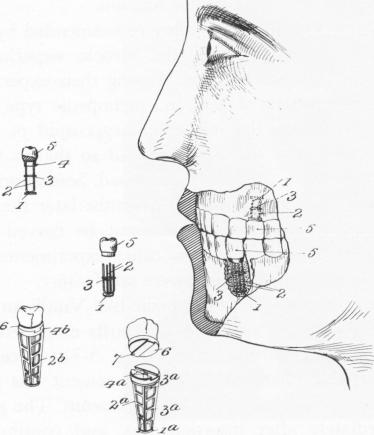
In 1901 Greenfield patented a "mounting for artificial teeth" (Fig. 5-2). This "mounting," now called an endosseous implant, was an iridioplatinum latticed cage whose transverse ribs were soldered to
Fig. 5-2. Greenfield's original patent, filed in 1909. Al-though the implant closely resembled a root in overall shape, it provided adequate space for tissues to grow into the implant itself.
upright bars. Atop this cage was a slotted disk into which a cap bearing an artificial tooth appropriate to the site could be cemented (Fig. 5-3) . Greenfield hoped that "in the course of time, the bone would grow in, around, and through the frame, and the latter would therefore be held securely in position so as to form a solid bearing for the tooth."*
Greenfield advised inserting his implant into a cavity in the jawbone drilled to the correct size and shape of the implant. In cases where a number of teeth were to be substituted, he planned to install two or more of these "bearing frames" at suitable positions and to bridge the teeth from one to another "in the manner well known to the art of dentistry." f
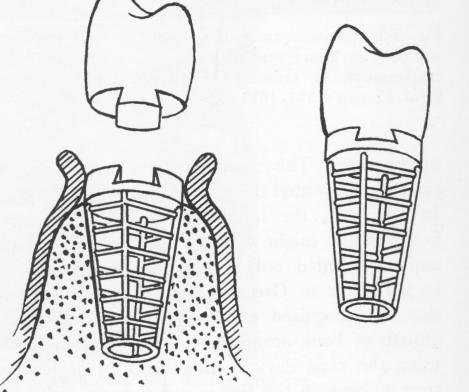
A few years later, in 1913, Greenfield modified his design and operative procedure. His revised implant was a cylinder with parallel sides (Fig. 5-4). He used a cylindrically shaped trephine the same size as the iridioplatinum cylinder to make a circular cut, leaving intact a core of bone over which the cylinder was placed. A roentgenogram of Green-field's 1913 implant shows the latticed cylinder in place (Fig. 5-5) .
Greenfield reported limited success. In at least one case his results were probably impeded by using one cylinder in the molar area and another in the canine area and suspending a gold bridge from one
*Greenfield, E. J.: Mounting for artificial teeth, U. S. Patent Office Serial No. 478,360, Patented Dec. 14, 1909. f Ibid.
Fig. 5-3. Another view of Greenfield's implant showing it in place. Note that the widest portion is at the alveolar crest.
|
|
Page 137 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|