| Theories and Techniques of Oral Implantology (vol.1) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
The evolution of dental implants 151
have been pulled out of shape because of the great resistance to pull provided by the deeper spires, which are firmly embedded in bone. To remove the em-bedded spires it was necessary to cut out a bone block (E). The close condensation of bone around the basal spires is obvious.
Other flaws in Formiggini's design are obvious today. Contrary to his idea, the number of spires is not the determining factor for their successful retention in bone, but rather their width, spacing, and depth (Fig. 5-28). Also, the uppermost spires in Formiggini's earliest implant were wider toward the surface of the alveolar crest than at the apex. This, plus the short neck that permitted these wide spires to lie close to the surface of the crest, invited the invagination of fibromucosal tissues and the subsequent loosening of the implant (Fig. 5-29). Formiggini himself, in his later designs, narrowed the wider uppermost spires and lengthened the neck. Other practitioners later designed implants whose spires were embedded well away from the alveolar crest.
F. Zepponi, a pioneer Italian implantologist working closely with Formiggini, was the first to cast a spiral implant.* The spirals and the abutment post were one unit, with the extratissular part modified for screwing on the prosthesis. Casting the spiraled implant was a great step forward. Because the implants were uniform in size and shape, planning a more exacting operative procedure was possible. The implant itself was sturdier, lessening the chance of creating weak points when bending the wire to fit a certain area.
Although a considerable improvement over Formiggini's hand-twisted spiraled implant, Zepponi's design still had flaws. One problem was the abutment post. Large enough to contain his screwing device, it was also large enough to put undue stress on the impact area. It is now known that the best designs are fashioned so that the impact is directed downward and dissipated throughout the implant. Also, because the abutment post was relatively short, the uppermost spirals were too close to the alveolar crest, inviting soft tissue invagination. How-ever many their faults, Zepponi's implants were still a step in the right direction.
After Formiggini, and well before all other European implantologists, Zepponi was the first to produce important histologic and macrographic
*Zepponi, F.: Protesi fisse a mezzo di infibulazioni endomascellari, Rev. Ital. Stomat., No. 1, 1955.
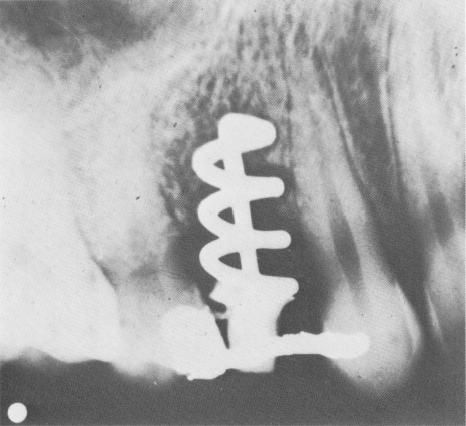
Fig. 5-29. A Formiggini implant failing because of the open spires close to the alveolar crest and the short neck. (From Chercheve, R.: Les implants endo-osseoux, Paris, 1962, Librairie Maloine.)
Fig. 5-30. Perron-Andres skillfully improved upon the Formiggini type implant. The spirals were fused to the abutment post. (From Linkow, L. I.: Clinical evaluation of various designed endosseous implants, J. Oral Implant Transplant Surg. 12:36, 1966.)

|
|
Page 151 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|