| Theories and Techniques of Oral Implantology (vol.1) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
166 Theories and techniques of oral Implantology
mandibular symphysis is very broad, with dense bone, Christensen made his transfixation screw heads very large with holes for smaller auxiliary screws.
To direct the pilot drill holes through the bone, Christensen also developed a special jig (Fig. 5-60). This instrument helps ensure that the drills emerge at the alveolar crest, not on the labial face of the bone, a fairly common occurrence when trying to set the screws parallel.
Christensen hospitalizes his patients and inserts the screws while the patient is under a general anesthetic. He incises all soft tissues—including the periosteum—over the inferior border of the mandible, reflects them, and applies the jig. He drills the holes, being careful to place them anterior to the mental foramina. When the holes have been drilled and irrigated, the jig is removed and the implants screwed into place with a special screwdriver. The
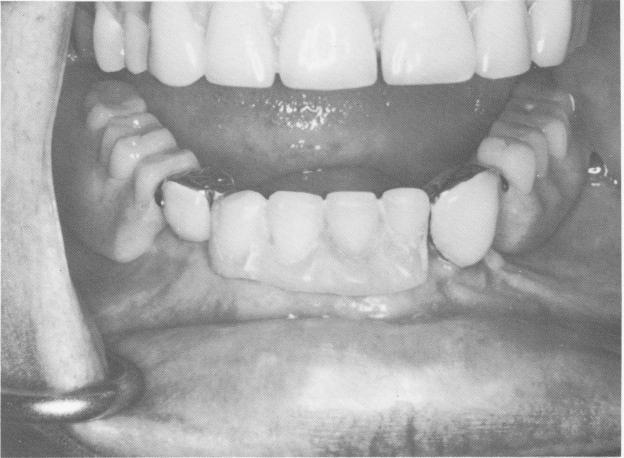
Fig. 5-62. Clinical view of the crowns over the protruding implant posts. (Courtesy R. V Christensen.)
Fig. 5-63. The denture is secured to the implant abutments. (Courtesy R. W. Christensen.)

|
|
Page 166 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|