| Theories and Techniques of Oral Implantology (vol.1) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
322 Theories and techniques of oral implantology
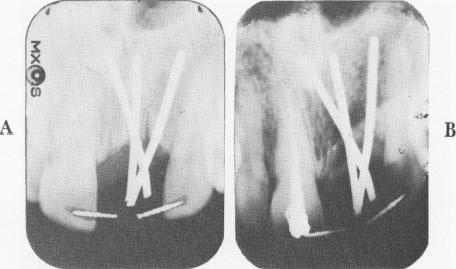
Fig. 8-38. A, Immediate postoperative radiograph. B, A postoperative radiograph taken 21 months later shows very little bone destruction. However, the thickness of the labial and palatal plates of bone camouflages the true picture of the medullary bone.
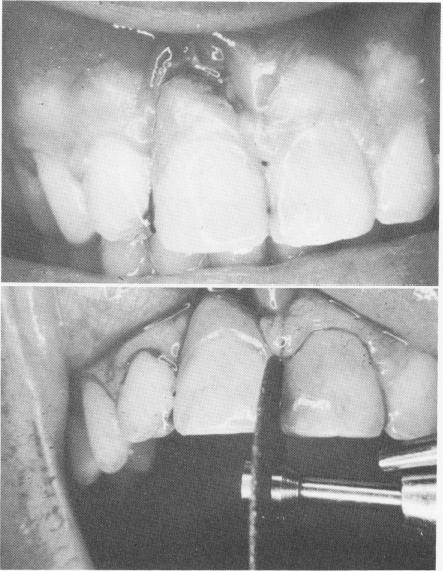
Fig. 8-39. A, Inflammation and hypertrophy are seen above the acrylic crown. B, With a carborundum disk, the wires of the A-splint are disked away on the mesial and distal aspect of the restoration, freeing it from its support.
Comparative results
The preceding cases, or minor variations of them, are fairly representative of the majority of presenting single tooth implantations. To learn more about the influence of stabilization on the success of single tooth implantations, Linkow set up four experimental groups. In Group I, the implant and
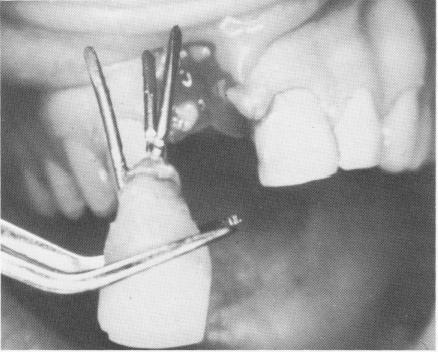
Fig. 8-40. The entire tripodial implant is removed with very little effort with the pins fused to each other and still di-verging from one another, with no fibrous tissue attached.
crown restoration were left completely independent of the neighboring teeth. In Group II, the implant and crown restoration were ligated immediately after insertion with dead soft .010 ligature wire to at least one or two neighboring teeth on both sides. In Group III, the implant was immobilized with tiny removable acrylic splints. In Group IV, the implant was A-splinted to its mesial and distal neighbors by channeling across the occlusal surfaces of the two natural teeth and the crown restoration and locking them together with a stainless steel or gold .036 wire sealed in place with acrylic.
For the first 72 to 90 hours, the implants in Group I were completely immobile. The patients had no pain and were able to masticate with all the pressure desired. However, in most cases the implants began to loosen after 90 hours. Soreness occurred around the apices of the implants and on the buccal, and sometimes the lingual, plates. Pain was felt if vertical forces were applied to the occlusal surfaces of the implant crowns. The mobility of the implant in many cases would range from a Class III and beyond. Some of the unsplinted implants did not loosen until about 7 or 8 days later, but then their sites went through the same rapid breakdown.
Once the Group I implants had loosened, a .010 dead soft ligature wire was used to ligate the loosened implant to a few teeth on each side of it. Almost immediately pain was eliminated and the patients were able to use the area to chew their food. The wire was left in place anywhere from 6 to 10 months with absolutely no discomfort to the patients. At the time the wire was removed, the
|
|
Page 322 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|