| Theories and Techniques of Oral Implantology (vol.2) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
468 Theories and techniques of oral implantology
an important role in resisting periodontal breakdown Because the blade is broad, it cannot be swiveled or its axis as can any post type implant.
-
The openings in the blades are much large] than those of the screw. Whereas such large opening: would weaken a post type implant, they have little effect on the strength of the wide body of the blade. The large openings allow a freer flow of blood carrying bone-rebuilding materials. Thus bone reconstruction is enhanced and retention of the implant improved.
-
Because the buccolingual width of the implant is quite narrow, the span between the alveolar bone walls is very short. Thus less bone needs to be re-generated to bind the implant. This means faster healing of the area where bone was depleted. Furthermore, the wedging of the blade into the viscoelastic environment of the bone appears to greatly stimulate osteogenesis.
-
A minimum amount of alveolar bone is sacrificed when surgically implanting the blade.
-
The threat of endangering anatomic land-marks, such as the mandibular canal with its con-tents and the maxillary sinus with its schneiderian membrane, can be reduced by shaping the blade to its site (Fig. 11-14). As long as a broad body is incorporated into the design, the implant may be manufactured or trimmed accordingly. The adverse consequences of perforating a maxillary sinus are also minimized by the blade's insertion technique. Because the blade is tapped into the bone and is broad and smooth, it merely pushes up the schneiderian membrane, rather than perforating it. Thus no pathway is created for drainage of the sinus' con-tents.
-
Because retention does not rely upon how deeply the implant is buried, as is the case with post type implants, blade-vents may be used in more sites. The broad anteroposterior length of the blade gives it stability. Thus in shallow areas a shallow blade may be used (Fig. 11-15). In extremely resorbed mandibles, blades have been successfully implanted buccally to a nearly dehiscent inferior alveolar nerve (Fig. 11-16).
-
There is very little opportunity for epithelial invagination below the shoulders of the blade because the mucosa, its underlying tissues, and the periosteum are completely incised down to the bone, retracted, and kept harmlessly away while the blade is implanted. Thus epithelial tissue cannot be pushed down into the implant site to form epithelial inclusions, such as can occur when using an implant that does not require soft tissue retraction.
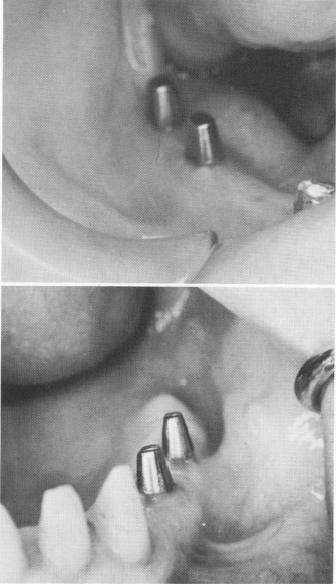
Afterward uncomplicated healing may take place as a result of the minimal amount of surgical trauma to the soft tissues. The healed soft tissues are extremely closely adapted, more so than those surrounding any other type of implant (Fig. 11-17).
Fig. 11-17. The soft tissues heal more firmly around the posts of a blade implant than around those of any other type of implant. This is a result of the blade's greater stability in bone.
Fig. 11-18. This radiograph clearly shows the suitability of the blade implant for knife-edge ridges.

|
|
Page 468 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|