| Theories and Techniques of Oral Implantology (vol.1) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
The evolution of dental implants 135
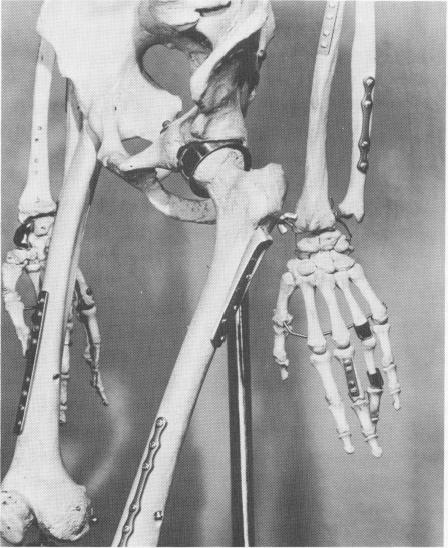
Fig. 5-1. Metallic prosthetic implantations have become common practice in orthopedics for fixing fractures and replacing parts of bone, joint surfaces, and even entire joints. Clinical experience has well established that metallic implants, especially those of cobalt-chromium alloys, are well tolerated in human tissue that heals in contact with them. (Courtesy Howmedica, Inc.)
were well tolerated by the tissues because they did not tend to ionize and therefore did not begin the chain of events leading to their eventual expulsion.
The inert metal recommended by Venable, Stuck, and Beach was Vitallium,* an alloy of cobalt, chromium, and molybdenum. Shortly thereafter Ticonium,f a nickel, cobalt, and chrome alloy, and tantalum were also shown to be relatively nonreactive electrolytically, although it is known today that nickel should not be included in the formula. In addition, it is now known that titanium is extremely well tolerated by the tissues.
The results of Venable, Stuck, and Beach's re-search stimulated considerable activity in orthopedics, and the inclusion of metallic pins, plates, and bars became even more common orthopedic practice (Fig. 5-1).
While the inclusion of metals for surgical repair
*Manufactured by Howmet Corp., New York.
(Manufactured by Consolidated Metals Products, CMP Industries, Chicago.
and as prostheses became more widespread in orthopedics, it did not in dentistry. Whereas in orthopedics the metallic inclusion was buried deep within the tissues, in dental implantology the metallic implant protruded from the tissues in which it was buried into the mouth. This supposedly invited infection along an open pathway into the bone. The body's primary defense mechanism against the invasion of disease-causing microorganisms—an unbroken layer of epithelium was apparently violated by a dental implant. However, it has been shown that in a well-healed site where the tissues lying under the projecting post are immobile, there is little inflammation or pocket formation; in fact, no more inflammation or irritation than is normal to a natural tooth has been found in successful implantations.
While dental implantologists were quick to perceive that the first objection to implants—intolerance of a foreign body by the tissues—might be easily overcome by using an inert metal, they en-countered a great deal of difficulty designing an implant that, after its insertion, would be almost entirely surrounded by bone, the most immobile of all tissues. Somehow, by a combination of design features and careful operative procedures, the invagination of oral epithelium had to be held to a minimum. This last criterion proved to be the major stumbling block in the history of implant design, for the considerations that must be taken into ac-count in achieving such a goal are complex and subtle.
Before surveying how various implant designs attempted to deal with or circumvent these difficulties, it is advisable to point out some of the major problems that must be solved in designing just one type of implant, the endosseous post type implant.
All post type implants consist of some kind of shaft or post whose major portion rests in bone and whose uppermost part protrudes through the oral epithelium into the mouth. This shaft or post may consist of one or more parts. To date the most functional designs consist either of one part or of several parts cast or fused together before insertion into the site. This is an obvious advantage, for it gives the implant greater strength, helping ensure against breakage, and makes the operative procedure less complicated.
The part embedded in bone should be irregularly shaped so that bone can grow into and through the irregularities. In the most functional implants, these irregularities are spaced widely enough that blood
|
|
Page 135 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|