| Theories and Techniques of Oral Implantology (vol.1) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
Operative tips 275
tuberosity area is as much as 6 or 7 mm. thick. Therefore either a blade with an exceptionally long neck should be used or the tissue should be thinned. With the blade in place, one flap is retracted and held with a hemostat or tissue forcep (Fig. 7-41), and the submucosal tissue is "degloved" with a scalpel (Fig. 7-42) . This is done until the underlying tissues are removed, leaving the surface tissues in-tact. These are approximated over the implant (Fig. 7-43) and sutured closed.
Paralleling the abutment post. The abutment post must be vertical to an imaginary horizontal plane and parallel to remaining teeth and implants. It should not interfere with occlusion. If it is necessary to angle the blade in bone so that the post is misaligned, the neck should be bent until the post
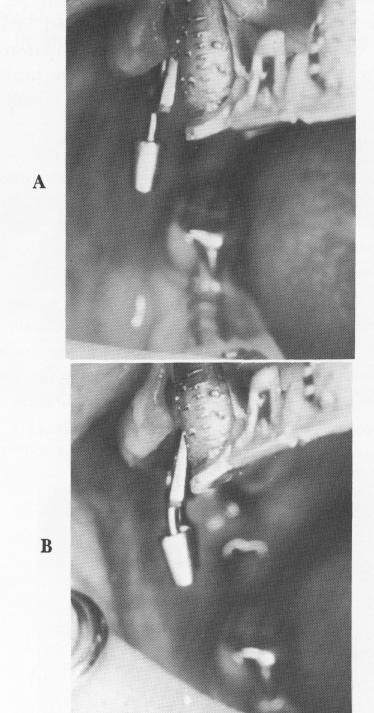
Fig. 7-45. An implant must never be bent in the mouth. A, It is tried in a groove and B, withdrawn so that it can be bent until its post is perpendicular to the anterior occlusal plane. The bent implant is then reinserted into the groove.
is correctly aligned. Therefore, before the blade is completely tapped into position, it is removed from the mouth. With two cone-socket pliers, one securing the bulk of the blade and the other gripping the post, the neck of the implant is bent buccolingually (Fig. 7-44) . The neck cannot be bent mesiodistally. Post preparation directly in the mouth accomplishes this. Fig. 7-45 shows such a case, with the post adjusted until it is perpendicular to the anterior occlusal plane.
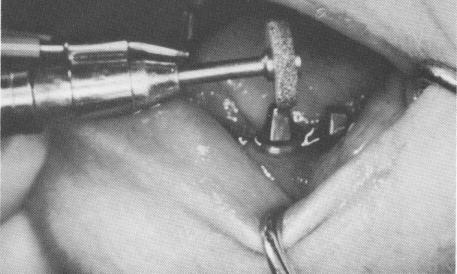
When bending the post is not adequate, further adjustments may be made in the mouth. To reduce a post's face, a fissure bur or tapered diamond stone with a water spray attachment may be employed. If the post is too tall, a heatless stone with a water attachment is used to shorten it (Fig. 7-46) .
Splinting. The immediate stabilization of blade implants after insertion with some form of temporary acrylic fixed splint has been carefully evaluated by Linkow. It is now his opinion that, unless needed for esthetic reasons, a splint is not necessary. In fact, there are advantages in leaving the site unsplinted. Because the soft tissues are exposed, the wound heals more rapidly. Also, there is no danger of irritation to or impingement on the soft tissues by a possibly ill-fitting temporary acrylic splint or prefabricated final prosthesis.
In cases where a prefabricated acrylic splint or a prefabricated palateless denture is constructed be-fore implant insertion in a completely edentulous maxilla, soft peripheral wax* is set inside the hollowed-out denture. After the denture is fitted over
*Surgident, Ltd., Los Angeles.
Fig. 7-46. To adjust occlusal height and attain mesial distal parallelism, a heatless stone with a water spray attachment and a tapered bur may be used.
|
|
Page 275 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|