| Theories and Techniques of Oral Implantology (vol.1) (published 1970) | Dr. Leonard I. Linkow |
|
|
Next Page |
| This is an archival HTML version of this book originally hosted here in 2006. The HTML may not display well on modern browsers. Please view the modern PDF Version for a better viewing experience. |
Operative tips 277
proaches the mental foramina, which also may be exposed, it should be made lingual to the foramen.
Exposing the bone. The periosteum should al-ways be cleanly separated from the underlying bone with little or no tearing to allow healing to take place uneventfully. The exposed bone should be constantly bathed with physiologic saline sponges while preparing for the surgical bone impression.
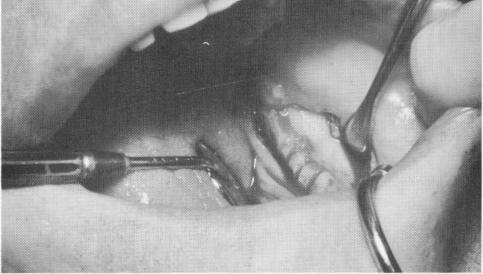
Making grooves. When using a unilateral or bilateral subperiosteal implant with lingual fingers, grooves must be made below the mylohyoid ridge. These grooves are easily prepared with a tapered diamond point used in a contra-angle with a water spray attachment. The prepared grooves should have no sharp line angles (Fig. 7-49), as they will round off from resorption. All debris resulting from making the grooves should be completely irrigated away before suturing.
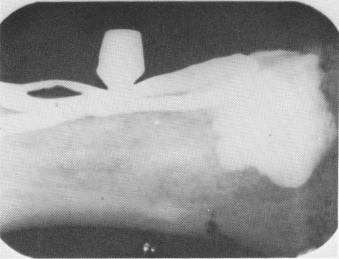
Taking impressions. Never leave any rubber base material under the mucoperiosteal tissues since it can be quite destructive to the bone (Fig. 7-50).
Fig. 7-49. Grooves prepared for the lingual fingers should be smooth and clean.
Fig. 7-50. All rubber base must be carefully removed after impression-taking. It contains a lead base that is detrimental to the bone and that appears radiopaque.
Before closing the tissues, careful irrigation and visual examination of the exposed jaw should be done.
Suturing. Suturing should be done so as not to create too much tension on the tissues closing the wound. If the tissues cannot be brought close together, then a horizontal accessory incision should be made between the sutures and the muscle attachments that lie below them. Similarly, if the healed tissues around the implant posts have re-ceded because of pulling caused by a high muscle attachment, a horizontal accessory incision should be made between the muscle attachment and the neck of the implant (Fig. 7-51) .
Oversuturing is preferable to undersuturing. Complete closure of the tissues is necessary to en-sure healing by primary intention.
Protecting the wound. After suturing the wound, it may be protected by an intraoral bandage (Fig. 7-52).
Preparing the remaining teeth. In cases where some anterior mandibular teeth are still present and a universal subperiosteal implant is the operator's choice, all periodontal work should be done either prior to or at the same time as taking the surgical impression. When the mucoperiosteal tissue is retracted in the area of the teeth, exposing bone and pocket depth, soft tissue pockets should be surgically removed and any bone overlying infrabony pockets should be leveled.
Fig. 7-51. A horizontal incision is sometimes necessary to release tension on the soft tissues around the implant post that is caused by high muscle attachments.

|
|
Page 277 |
Next Page |
|
Copyright warning: This information is presented here for free for anyone to study online. We own exclusive internet copyrights on all content presented on this website. We use sophisticated technology to identify and legally close down websites that reproduce copyrighted content without permission - so please don’t do it.
|